Cardiomyopathy
•
39 likes•9,389 views

Cardiomyopathy refers to disease of the heart muscle or electrical dysfunction. the Causes of cardiomyopathy are classified as PRIMARY or SECONDARY

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Cardiomyopathy
Similar to Cardiomyopathy (20)
More from ANILKUMAR BR
More from ANILKUMAR BR (20)
Recently uploaded
Recently uploaded (20)
Cardiomyopathy
- 2. CARDIOMYOPATHY Cardiomyopathy refers to disease of the heart muscle or electrical dysfunction.
- 4. CAUSES Causes of cardiomyopathy are classified as PRIMARY or SECONDARY 1. Primary cardiomyopathies have genetic, mixed, or acquired etiologies. 2. Secondary cardiomyopathies have infiltrative, toxic or inflammatory causes
- 5. Types of cardiomyopathies Cardiomyopathies classified according to the structural abnormalities of the heart muscle. 1. Dilated cardiomyopathy (DCM) 2. Hypertrophic cardiomyopathy (HCM) 3. Restrictive or Constrictive cardiomyopathy (RCM) 4. Arrhythmogenic right ventricular cardiomyopathy (ARVC) and unclassified cardiomyopathy
- 6. Etiopathophysiology Dilated cardiomyopathy (DCM) : Dilated cardiomyopathy is the most common form of cardiomyopathy. It can be divided into two types ischemic and non ischemic cardiomyopathy. 1. ischemic cardiomyopathy : a) It is caused by inadequate oxygen supply due to obstruction in coronary artery. b) The lack of oxygen interrupts both mechanical &electrical function of the cells , decrease contractility , and causes dysrhythmias.
- 7. 2) Non ischemic cardiomyopathy: a) Cause id idiopathic ( unknown) b) 10 to 50 % of cases are identified by genetic mutation c) Both the RV & LV enlarge significantly, causing a decrease in the ability of the heart to pump blood efficiently to the body.
- 8. Dilated cardiomyopathy (DCM) Alcohol abuse Chemotherapy Chemical agents Myocarditis Pregnancy ( third trimester & postpartum) Valve disease, endocrine disorders, and infections such as HIV can cause dilated cardiomyopathy.
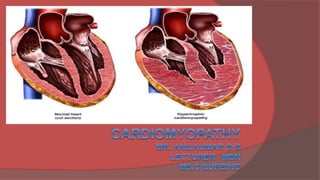
- 9. Hypertrophic cardiomyopathy (HCM) Hypertrophic cardiomyopathy is a genetically transmitted disorders. Hypertrophic cardiomyopathy is primarily due to the abnormal thickening of the ventricular septum of the heart. The thickened heart muscle & ultrastructure disruption change the shape, size, & dispensability of the ventricular cavity & alter the normal thickens & functioning of the mitral valve; as a result, the heart ability to relax & contract normally is impaired.
- 10. Restrictive or Constrictive cardiomyopathy (RCM) The heart muscle becomes infiltrated by various substances , resulting in severe fibrosis. The heart muscle becomes stiff and non distensible, impairing the ability of the ventricle to fill with blood adequately.
- 11. Arrhythmogenic right ventricular cardiomyopathy Autosomal genetic disorder affects 1 in 2,000 to 5,000 more common among men Arrhythmogenic right ventricular cardiomyopathy characterized by placement of the RV myocytes by fibro-fatty tissue, RV dysfunction, & ventricular dysrhythmias.
- 12. Complications of cardiomyopathy CHF Ventricular dysrhythmias Atrial dysrhythmias Cardiac conduction defects Pulmonary or cerebral embolism Valvular dysfunction Pulmonary embolism Sudden cardiac death
- 13. Clinical manifestations Patients with cardiomyopathy may remain stable and without symptoms for many years, As the disease progress, so do symptoms.
- 14. Clinical manifestations Frequently Dilated cardiomyopathy or Restrictive cardiomyopathy is first diagnosed when the patient presents with sings and symptoms of heart failure ( dyspnea on exertion, fatigue) Patients with cardiomyopathy may also report PND, Cough, and orthopnea, which may lead to misdiagnosis of bronchitis or pneumonia. Other symptoms include fluid retention, Peripheral edema, and nausea The patient also may experience chest pain, palpitations, dizziness, and syncope
- 15. other common clinical manifestations Exertional dyspnea Chest pain Signs of HF Pulmonary edema Dysarhythmias Pericardial effusions Cardiac murmur Sudden cardiac death may be the first sign with Arrhythmogenic right ventricular cardiomyopathy
- 16. Assessment and diagnostic Evaluation History collection(History of the disease in immediate family members) Cardiovascular examination Chest X-ray ( for cardiomegaly) ECG (may show dysrhythmias) Echocardiogram (The echocardiogram is one of the most helpful diagnostic tools because the structure and function of the ventricles can be observed easily.) Cardiac catheterization ( to help diagnose ischemic or non- ischemic)
- 17. Management client with cardiomyopathy The goal of management is to maximize ventricular function and prevent complications associate with cardiomyopathy.
- 18. Management client with cardiomyopathy Medical management is directed toward determining and managing possible underlying causes, correcting the heart failure with medications, a low – Sodium diet, and an exercise /rest regimen and controlling dysrhythmias with anti arrhythmic medications and possibly with an implanted electronic devices, such as an implanted cardioverter defibrillator (ICD) .
- 19. Management client with cardiomyopathy Infective endocarditis prophylaxis and systematic anticoagulation to prevent thromboembolic events are usually recommend. The person with HCM may also have to limit physical activity to avoid a life-threatening dysrhythmia. A pacemaker may be implanted to alter the electrical stimulation of the muscle and prevent the forceful hyperdynamic contractions that occur with HCM
- 20. Surgical Management client with cardiomyopathy When heart failure progresses and medical treatment is no longer effective, surgical intervention, including heart transplantation, is considered. However, because of the limited number of organ donors, many patients die waiting for transplantation. In some cases, a Left ventricular assist device (LVAD) is implanted to support the failing heart until a suitable donor heart becomes available.
- 21. Left ventricular assist device (LVAD) A left ventricular assist device, or LVAD, is a mechanical pump that is implanted inside a person's chest to help a weakened heart pump blood.
- 22. Left ventricular assist device (LVAD)
- 23. Left ventricular assistive device ( LVAD)
- 24. Left Ventricular Outflow Tract Surgery. The most common procedure is a Myectomy (sometimes referred to as a Myotomymyectomy), in which some of the heart tissue is excised. Septal tissue approximately 1 cm wide and deep is cut from the enlarged septum below the aortic valve. The length of septum removed depends on the degree of obstruction caused by the hypertrophied muscle.
- 25. Left Ventricular Outflow Tract Surgery. The primary complication of both procedures is dysrhythmia; additional complications are postoperative surgical complications such as: Pain Ineffective airway clearance Deep vein thrombosis (DVT) Risk for infection and delayed surgical recovery.
- 26. Heart Transplantation. The first human-to-human heart transplant was performed in 1967. Since then, transplant procedures, equipment, and medications have continued to improve. heart transplantation has become a therapeutic option for patients with end-stage heart disease.
- 27. Heart Transplantation Techniques. Orthotopic transplantation : is the most common surgical procedure for cardiac transplantation. The recipient’s heart is removed, and the donor heart is implanted at the vena cava and pulmonary veins.
- 28. Heart Transplantation Techniques. Heterotopic transplantation: is less commonly performed .The donor heart is placed to the right and slightly anterior to the recipient’s heart; the recipient’s heart is not removed.
- 29. Postoperative Course Heart transplant patients are constantly balancing the risk of rejection with the risk of infection. They must comply with a complex regimen of diet, medications, activity, follow-up laboratory studies, biopsies (to diagnose rejection), and clinic visits. Most commonly, patients receive cyclosporine or tacrolimus (FK506, Prograf), azathioprine (Imuran) or mycophenolatemofetil (CellCept), and corticosteroids (ie, prednisone) to minimize rejection.
- 30. Mechanical Assist Devices and Total Artificial Hearts Ventricular Assist Devices ( VAD) . More complex devices that actually perform some or all of the pumping function for the heart also are being used. Total Artificial Hearts. Total artificial hearts are designed to replace both ventricles. Some require the removal of the patient’s heart to implant the total artificial heart; others do not.
- 31. Nursing management: patient with cardiomyopathy Nursing assessment for the patient with cardiomyopathy begins with a detailed history of the presenting signs and symptoms. The nurse identifies possible etiologic factors, such as heavy alcohol intake, recent illness or pregnancy, or history of the disease in immediate family members
- 32. Nursing management: patient with cardiomyopathy Evaluate clients chief complaint, which may include chest pain, fever, syncope, general aches, fatigue, dyspnea. Evaluate etiologic factors , such as alcohol abuse, pregnancy, recent infection, or history of endocrine disorders. Assess for positive family history Auscultate lung sounds for crackles ( pulmonary edema) or decreased sound (Pleural effusion) Evaluate cardiac rhythm & ECG for evidence of atrial or ventricular enlargement or infection.
- 33. Nursing management: patient with cardiomyopathy The physical assessment focuses on signs and symptoms of congestive heart failure. The baseline assessment includes such key components as: Vital signs Calculation of pulse pressure and identification of pulsus paradoxus Current weight; determination of weight gain or loss Detection by palpation of the point of maximal impulse, often shifted to the left
- 34. Nursing management: patient with cardiomyopathy Cardiac auscultation for a systolic murmur and third and fourth heart sounds Pulmonary auscultation for crackles Measurement of jugular vein distention Identification of presence and severity of edema
- 35. NURSING DIAGNOSES Decreased cardiac output related to decreased ventricular function and /or dysrhythmias. Ineffective cardiopulmonary, cerebral, peripheral, and renal tissue perfusion related to decreased peripheral blood flow (resulting from decreased cardiac output). Impaired gas exchange related to pulmonary congestion caused by myocardial failure (decreased cardiac output). Activity intolerance related to decreased cardiac output or excessive fluid volume, or both.
- 36. NURSING DIAGNOSES Anxiety related to fear of death, surgical procedures, and hospitalization. Noncompliance with medication and diet therapies
- 37. Nursing interventions Improving cardiac output Increasing activity tolerance Reducing anxiety
- 38. Patient education and health maintenance Teaching Patients Self-Care :Teaching patients about the medication regimen, symptom monitoring, and symptom management is a key part of the plan of nursing care.