
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Cystic neoplasm of pancreas
Similar to Cystic neoplasm of pancreas (20)
More from Anupshrestha27
More from Anupshrestha27 (11)
Recently uploaded
Recently uploaded (20)
Cystic neoplasm of pancreas
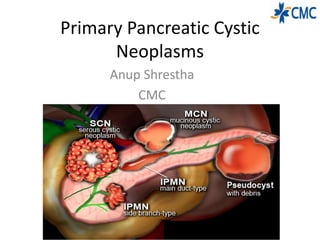
- 1. Primary Pancreatic Cystic Neoplasms Anup Shrestha CMC
- 2. History • Becourt in 1830.
- 3. Introduction • Cystic neoplasms of the pancreas are the heterogenus group of cystic lesions and remain a diagnostic challenge. • While the incidence of these lesions increases, so does the differential diagnosis. • Management decisions are extremely difficult due to the uncertain biologic behavior of these lesions.
- 4. Klöppel’s Classification of Cystic Neoplasms of the Pancreas
- 5. • The three most common types of PCNs are serous cystic neoplasms (SCNs), mucinous cystic neoplasms (MCNs), and IPMNs, representing approximately 90% of all PCNs. • MCNs and IPMNs are the most common and more importantly have the highest potential for malignant transformation. • SCNs occur much less frequently and are almost always benign.
- 6. SEROUS CYSTIC NEOPLASMS(SCN) • described as multilobulated multiloculated cystic masses with central stellate scars and calcifications • SCNs are most commonly observed in women (3 : 1 female to male ratio) There are four subtypes of SCNs: • serous microcytic adenoma • serous macrocytic (oligocystic) adenoma • von Hippel-Lindau (VHL)-associated pancreatic cysts • serous cystadenocarcinoma.
- 7. Pathology • SCNs are characterized by serous fluid–filled cysts lined by a single layer of cuboidal epithelial cells with uniform, round, darkly stained nuclei and a glycogen-rich cytoplasm. • Notably, there is a lack of atypia, necrosis, and mitotic features in SCNs. • On gross examination, microcystic SCNs have a characteristic honeycomb appearance with multiple thin- walled cysts around a central scar
- 8. Von Hippel-Lindau–Associated Pancreatic Cysts • VHL disease is an autosomal dominant mutation of chromosome 3p25 causing multiorgan pathology. VHLassociated pancreatic cysts show a loss of heterozygosity on chromosome 3p25 and mutations in the VHL gene. • These lesions are indistinguishable from sporadic serous cystadenomas. In contrast, VHL patients tend to have multifocal disease rather than a single lesion. These lesions behave similarly to non-VHL serous cystadenomas with minimal malignant potential.
- 9. Serous Cystadenocarcinoma • Malignant SCNs are exceedingly rare • Serous cystadenocarcinomas are misdiagnosed as a malignancy due to the presence of vascular impingement on imaging. • These malignant cysts are nearly identical to benign serous cystadenomas and are distinguished only by the presence of metastases
- 10. Imaging • Three different imaging patterns exist for SCNs: microcystic, honeycomb, and oligocystic 1.Microcystic
- 13. MRI • SCNs on MRI appear as a “cluster of grapes” on T2- weighted images with multiple small cysts and enhanced septations. • The presence of bright T1- weighted cystic fluid suggests hemorrhagic fluid content. • The main disadvantage of MRI is the inability to detect central calcifications commonly seen with SCNs
- 14. EUS-FNA and Cytology EUS • SCNs typically appear as microcystic compartments with the absence of fluid. • Some SCNs have macrocystic components that can resemble MCNs. Cytology • For cytological assessment and cyst fluid drainage, in order to distinguish between serous and mucinous lesions • The cytology of SCNs includes bland cuboidal cells containing glycogen, clear cytoplasm without cellular atypia or necrosis
- 15. Treatment and Survillence • Asymptomatic patients with radiological evidence of an SCN should be followed up for 1 year. • When the diagnosis of SCN is clear, surgery is recommended only in patients with symptoms related to the compression of adjacent organs (ie, bile duct, stomach, duodenum, portal vein) • Other indications include cyst size greater than 4 cm and uncertainty of diagnosis despite appropriate radiologic assessment • enucleation of the cyst. • Avoid Enucleation : is associated with high morbidity (approximately 40%) due to the development of a pancreatic fistula
- 16. MUCINOUS CYSTIC NEOPLASMS • The average age range of presentation is 40 to 50 years old • they are found predominantly in perimenopausal women (20 : 1 female-to- male ratio). • The vast majority of MCNs are found in the body and tail of the pancreas. • Most MCNs are approximately 6 to 10 cm at the time of diagnosis but range from 1.5 to 35 cm in diameter. • On gross examination, they are spherical and infrequently encapsulated by a calcified fibrous wall. • The cyst can be filled with mucin, blood, or a watery fluid. This fluid tends to be thicker and more viscous than in SCN, due to the presence of mucus. MCNs do not communicate with the pancreatic ductal system
- 17. MCN- Histology • MCNs are lined by tall mucin- producing columnar cells. • These epithelial cells that line the cyst may be papillary or flat and can show a tendency toward gastric or intestinal differentiation. • Ovarian-like stroma is a histologic feature often seen • in MCN.
- 18. MCN-Malignant Potential • three distinct categories based on the degree of cellular atypia: low-, intermediate-, and high-grade. • The classification is based on the greatest degree, and not the average, of the epithelial dysplasia. • Less than 20% of MCNs are associated with invasive carcinoma and thus should be considered a potential precursor to pancreatic cancer. • Extensive sampling of the cyst is recommended, given the relatively small volume of the invasive component. It appears that the incidence of malignant transformation is directly correlated to the overall size of the cyst and the complexity of the cyst.
- 19. Imaging-CT (A) Macrocystic form: note septum and lack of surrounding inflammatory reaction. (B) Several macrocystic areas (>2 cm) in midbody of pancreas.
- 20. MRI • well-defined, uniloculated or multiloculated cystic lesion(s) with enhanced septations and occasionally solid components.. • High signal intensity on T1- and T2-weighted imaging can result from mucin within the cyst. • The proximity of the cyst to the ductal system is better assessed with MRI and can help to differentiate MCNs from pseudocysts and IPMNs.
- 21. Cystic Fluid Analysis • The presence of mucin is highly specific for MCNs • Most MCNs contain higher concentrations of CEA compared with their SCN counterparts (>192ng/mL)
- 22. Treatment and Survilence • MCN ≥40 mm should undergo surgical resection. • Resection is also recommended for MCN which are symptomatic or have risk factors (ie, mural nodule) irrespective of their size • MCN measuring <40 mm without a mural nodule or symptoms may undergo surveillance with MRI, EUS, or a combination of both. Surveillance is recommended every 6 months for the first year, then annually if no changes are observed
- 23. INTRADUCTAL PAPILLARY MUCINOUS NEOPLASMS IPMNs are defined in the WHO Classification of Tumors of the Digestive System as an intraductal, grossly visible epithelial neoplasm of mucin- producing cells. Using imaging and histology, IPMNs can be classified into three types based on duct involvement: 1. Main-duct IPMN (approximately 25% of IPMNs): Segmental or diffuse dilation of the main pancreatic duct (>5 mm) in the absence of other causes of ductal obstruction. 2. Branch-duct IPMN (approximately 57% of IPMNs): Pancreatic cysts (>5 mm) that communicate with the main pancreatic duct. 3. Mixed type IPMN (approximately 18% of IPMNs): Meets criteria for both main and branch duct.
- 24. Pathology • IPMN lesions are characterized by papillary projections of columnar- lined epithelium with varying degrees of dysplasia. • Mucin is typically abundant both within the cytoplasm of the lining epithelial cells as well as within the acellular fluid matrix
- 25. Intraductal Papillary Mucinous Neoplasm–Associated Malignancy • Invasive cancer is found in 20% to 50% of resected IPMN specimens Factors shown to be associated with the presence of invasive cancer • jaundice at presentation • larger lesions (≥ 30mm) • mural nodules (≥5 mm) • main-duct dilation ≥10 mm • serum cancer antigen (CA) 19-9 levels
- 26. Risk of high-grade dysplasia or malignancy according to dilatation of the main pancreatic duct in IPMN The European Study Group on Cystic Tumours of the Pancreas. Gut 2018;67:789–804.
- 27. Genetics of Intraductal Papillary Mucinous Neoplasm • Similar to the genetic landscape of pancreatic cancer, KRAS mutations, loss of p16, and TP53 mutations are frequently observed in IPMN • SMAD4/ DPC4 expression, which is inactivated in more than half of patients with pancreatic adenocarcinoma, is preserved in virtually all noninvasive IPMNs. • Another prominent difference is the mutations of the GNAS gene in IPMN.
- 28. Clinical presentation Presentation: • Abdominal pain. • Pancreatitis. • Weight loss. • Jaundice. • New onset diabetes. Investigation • variable amylase level • a high CEA level (>200 ng/mL) • CT Scan characteristics: • Main pancreatic or duct dilation. • Involvement of any part of the pancreas or the whole pancreas. • Continuity of cyst with ductal system. • Irregular and poorly demarcated
- 29. MRCP and EUS • MRCP may actually be better than CT for determining a communication with the pancreatic duct and thus in diagnosing branch-duct IPMN • Careful evaluation with EUS can provide detailed images of the cyst wall and internal cyst architecture. Fine-needle aspiration and biopsy can be performed with EUS.
- 30. EUS
- 31. Treatment of MD-IPMN • Indications for Surgery
- 32. Extent of Resection • Limited to a part of the pancreas and there is no overt radiographic evidence of malignancy resection of the IPMN-containing pancreas, with pancreaticoduodenectomy for the head of the pancreas • distal pancreatectomy for the body and tail of the pancreas. • Patients with MD-IPMN diffusely involving the whole gland pose a difficult management dilemma. • In cases in which there is a mural nodule within the MPD further along the duct, or in patients with an increased risk for malignancy (ie, patients with familial pancreatic cancer), a total pancreatectomy can be considered • MT-IPMN carries a risk of malignant transformation that is comparable to MD-IPMN, and resection is therefore advised in patients who are fit for surgery
- 33. Resection of BD-IPMN Tanaka M, Fernández-del Castillo C, Adsay V, Chari S, Falconi M, Jang J-Y, et al. International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology. 2012 Jun;12(3):183–97 High-risk stigmata of malignancy • Obstructive jaundice in a patient with a cystic lesion in the head of the pancreas • Enhancing mural nodule ≥ 5 mm • Main pancreatic duct ≥ 10 mm in size Worrisome clinical features • Pancreatitis Worrisome imaging features • Cyst ≥ 3 cm • Enhancing mural nodule < 5 mm • Thickened/enhancing cyst walls • Main duct size 5–9 mm • Nonenhancing mural nodule • Abrupt change in caliber of pancreatic duct with distal pancreatic atrophy • Lymphadenopathy • Increased serum level of CA-19-9 • Cyst growth rate ≥ 5 mm / 2 years Resection without further investigation Should undergo further evaluation with EUS
- 34. Survillence
- 35. Types of Surgery • Branch-duct lesions in the head of the pancreas are resected with pancreatoduodenectomy • In the tail, distal pancreatectomy with or without splenectomy. • Recently, pancreas-sparing procedures, such as enucleation and central pancreatectomy, have been reported in an effort to maintain the exocrine and endocrine pancreatic function • Total pancreatectomy is reserved for fit patients with diffuse MD- IPMN
- 36. Reference • European evidence-based guidelines on pancreatic cystic neoplasms (The European Study Group on Cystic Tumours of the Pancreas) • BLUMGART’S Surgery of the Liver, Biliary Tract, and Pancreas (6th edition) • Shackelford’s SURGERY Of The ALIMENTARY TRACT( 8th Edition) • The many faces of pancreatic serous cystadenoma: Radiologic and pathologic Correlation L.C. Chu et al. Diagnostic and Interventional Imaging (2017) 98, 191—202
- 37. Thank You
Editor's Notes
- walls“I have actually found that the first cystic tumor of pancreas to be described was in a french journal in It was described as a mass in a size of a child’s head composed of very strong fibrous walls.
- Incidental finding in 2 % of the abdominal imaging
- Klöppel and colleagues classified the lesions
- The cystic spaces do not communicate with the pancreatic ductal system. The surrounding stroma usually contains nerves, islets, lymphoid aggregates, and vascular channels
- (a.). Arterial phase CECT image shows an infiltrative, heterogeneous, predominantly hypervascular mass involving the pancreatic body (white arrows) and several hypervascular lesions in the liver. (b.). Portal phase image shows ductal dilation and parenchymal atrophy in the pancreatic tail (black arrow), as well as peripancreatic lymphadenopathy (black arrowhead) and collateral circulation (black arrow) secondary to splenic vein thrombosis. (c.). Portal phase image shows splenic vein (white arrow) thrombosis secondary to tumor infiltration by the pancreatic mass (black arrowhead); some of the liver lesions are shown to have necrotic center (black arrow). (d.). Delayed phase shows contrast washout of the liver lesions (black arrows).
- microcystic mass within tail of pancreas with characteristic central stellate scar with calcifications (arrow) and thin internal enhancing septations (arrowhead
- Shows lobulated spongiform mass (arrow) with poor visualization of individual microcysts; b: gross pathology photograph illustrate numerous microcysts in the honeycomb pattern
- shows a thin-walled cystic masswithin tail of pancreas with minimally lobulated outer margin (arrow); b: gross pathology photograph shows an oligocystic mass wrappingaround a mildly dilated pancreatic duct without direct communication with the pancreatic duct (
- MRI is able to detect very small cysts due to superior soft tissue contrast resolution compared with CT. Top left, T1-weighted image; top right, T2-weighted image; bottom left, T1-weighted gadolinium-enhanced image; bottom right, fat-suppressed T1-weighted gadolinium-enhanced image. The mass is externally lobulated and hypointense on the T1-weighted image and hyperintense on the T2-weighted image, with septal enhancement
- The presence of the microcystic appearance usually does not warrant FNA due to the benign nature of disease. The main limitation of FNA is the nondiagnostic result due to a lack of adequate cellular material, causing a potential false-negative to occur
- MCNs are cystic tumors of the pancreas that have a lower incidence than serous cysts or IPMNs. Almost all MCNs are multiloculated.
- The stroma of the ovary is a unique type of connective tissue abundantly supplied with blood vessels, consisting for the most part of spindle-shaped stroma cells. These appear similar to fibroblasts. The stroma also contains ordinary connective tissue such as reticular fibers and collagen. Ovarian stroma differs from typical connective tissue in that it contains a high number of cells. The stoma cells are distributed in such a way that the tissue appears to be whorled. Stromal cells associated with maturing follicles may acquire endocrine function and secrete estrogens. The entire ovarian stroma is highly vascular. Staining for estrogen and progesterone is positive in most cases. Frequently seen in young women, the mean age at presentation is in the fifth decade
- In 2010 the World Health Organization (WHO) classification divided
- MRI is able to better identify the contents of the cyst compared with CT imaging a large oligocystic lesion arising from the pancreatic body/tail (arrowhead = septation, thick arrow = small locule); (B) delayed-phase image shows very faint enhancement of thin walls of septum and locule. Splenic vein occlusion confirmed by the large, tortuous venous collaterals along the tumor margin (long arrow).
- Due to the malignant potential of MCNs, it is generally recommended that these lesions be resected To avoid incomplete treatment of invasive carcinoma, a standard oncologic resection (distal pancreatectomy in 90–95% of MCN) with lymph node dissection and splenectomy is indicated for any MCN with imaging features indicating high-grade dysplasia or cancer ( Some case reports have suggested considerably faster growth of MCN during pregnancy, potentially leading to tumour rupture. Therefore, patients with MCN should be observed closely during pregnancy.
- IPMNs are commonly found in the uncinate process
- IPMN into the categories of low-grade dysplasia, moderate dysplasia, high-grade dysplasia, and carcinoma
- Malignancy arising from IPMN is well documented, and several large series have been reported in the literature (Ajani et al, 2010; D’Angelica et al, 2004; Nara et al, 2009; Salvia et al, 2004; Schnelldorfer et al, 2008; Sohn et al, 2004; Woo et al, 2009). The presence of a cyst size ≥30 mm, without any other radiological or clinical risk factors, has a positive predictive value for malignancy of between 27% and 33%.Patients with an IPMN measuring ≥30 mm have a 5% risk of developing malignancy, from which they will die within 3 years, whereas the 5 years disease-free survival after resection of IPMN is 96%.
- Although IPMN shares many molecular alterations with pancreatic cancer, there are some significant differences with respect to both the incidence of these mutations as well as the presence of novel mutations p16is a protein that slows cell division by slowing the progression of the cell cycle from the G1 phase to the S phase, thereby acting as a tumor suppressor. The TP53 gene provides instructions for making a protein called tumor protein p53 (or p53). This protein acts as a tumor suppressor, which means that it regulates cell division by keeping cells from growing and dividing (proliferating) too fast or in an uncontrolled way
- variable amylase level, reflecting communication with the pancreatic duct, and a high CEA level (>200 ng/mL) Main-duct IPMN with involvement of the entire main pancreatic duct. Branch-duct IPMN.L
- BD-IPMN - note the connection of the lesion via a branch duct to the main duct; the arrowhead points at the BD from which the IPMN arises. Careful evaluation with EUS can provide detailed images of the cyst wall and internal cyst architecture. Fine-needle aspiration and biopsy can be performed with EUS and may include both biopsy of the cyst and aspiration of cyst fluid for cytology and analysis for tumor markers
- EUS showing hyperplastic or a polypoid growth of the epithelial layer (arrows) and hyperechoic ductal margin (arrow heads) of the irregularly dilated main pancreatic duct.
- Because these lesions have a high risk of harboring high-grade dysplasia or invasive disease. Even when malignancy or high-grade dysplasia does not exist at the time of presentation, it is believed that most, if not all, MD-IPMNs will progress to malignancy These recommendations also apply to mixed variants, because there appears to be a similar incidence of high-grade dysplasia or invasive disease whenever the main duct is dilated
- When performing partial pancreatectomy for IPMN, intraoperative frozen-section evaluation focused on the identification of high-grade dysplasia or an occult invasive cancer at the margin should be performed Ductal dilation throughout the pancreas could be due to MD-IPMN extending throughout the pancreatic duct or due to outflow obstruction caused by malignancy or IPMN in the head of the pancreas.
- Revised international consensus guidelines for the management of IPMN and MCN of the pancreas have classified the concerning radiographic features into “worrisome features” and “high-risk stigmata