Dynamic hip screw
•
165 likes•36,046 views

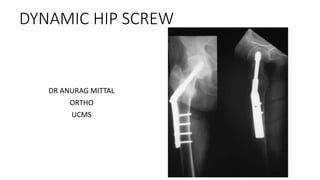
DYNAMIC HIP SCRE SURGERY FOR INTERTROCHANTERIC FRACTURES

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Dynamic hip screw
Similar to Dynamic hip screw (20)
More from Dr. Anurag Mittal
More from Dr. Anurag Mittal (18)
Recently uploaded
Recently uploaded (20)
Dynamic hip screw
- 1. DYNAMIC HIP SCREW DR ANURAG MITTAL ORTHO UCMS
- 2. INDICATION • Stable intertrochanteric fracture till 2.1 –study by evans and another by Hornby-non operative vs operative • Low complication ,mortality rate,pain, leg swelling, sores –same in both • But shorter hospitalization • Better restoration of normal anatomy • Ability to live independently • Basicervical neck of femur # with derotation screw • Unstable # with • TSP • Axial dynamic compression plate • IHS
- 5. TSP
- 7. IHS
- 8. Principle • Controlled collapse • Dynamic action reduces incidence of screw cut out and penetration of screw into hip joint
- 9. Procedure
- 10. Position
- 11. Reduction • Undisplaced #-no reduction,slight IR • Displaced#- • extension , • Abduction-corrects varus • IR –”screw home” the distal fragment • Evaluation • #displacement • Neck shaft angle • Anteversion • Femoral shaft ‘sag’ • Rotation checked clinically
- 12. Lateral approach to the proximal femur
- 13. Guide pin insertion • For 135 angled plate • If higher angled plate-entry moved 5 mm distally for 5 degree increase
- 14. ANGLE GUIDE
- 17. • Why 135 ideal?? • Hip joint resultant force-159- difficult insertion/cut out • 130-high bending load • Influence of nail plate angle on bending moment: Larger angle results in smaller moment because of shorter distance (d); conversely, smaller angle results in larger moment because of longer distance
- 18. TIP APEX DISTANCE • Should be <25mm • Tip of screw should lie under 10 mm of subchondral bone • Screw should ideally lie in centre on ap and lateral views • Superior and anterior location avoided-cut out
- 19. Lag screw length • Measuring guide used • Tip extension and immediate telescoping must be taken into account
- 20. Short vs long barrel • <85 mm—short barrel • >=85 mm—standard barrel • WHY?? • Thread length-22mm • Recommended sliding -25 mm(min 10 mm) • Standard barrel length-38 mm(short-25 mm) • So 22+25+38=85mm
- 21. COMPONENTS SHORT BARREL LONG BARREL TRIPLE REAMER
- 25. Implant insertion and fixation • Long vs short side plate • More dissection • Complicate future surgery • no improvement in proximal purchase • Inherent stability of fracture/reduction not altered • Reduces tensile forces on prox two screws but no additional protection • Same rate of failure
- 26. Keyed system
- 31. • Traction released • Angled plate acts as an aid to reduction • Intraop prox displacement of femoral shaft along the plate before screw insertion • Post op as lag screw collapses into the barrel by impaction • Compression screw-also prevents postop hip screw barrel disengagement
- 32. Complication
- 33. •