
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Primary spaces of space infection
Similar to Primary spaces of space infection (20)
Recently uploaded
Recently uploaded (20)
Primary spaces of space infection
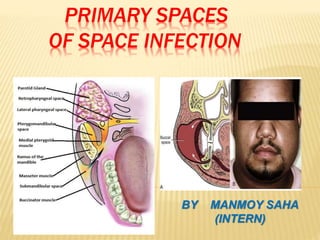
- 1. PRIMARY SPACES OF SPACE INFECTION BY MANMOY SAHA (INTERN)
- 2. CONTENTS INTRODUCTION POTENTIAL SPACES PRIMARY MAXILLARY SPACES -CANINE SPACE -BUCCAL SPACE -INFRA TEMPORAL SPACE PRIMARY MANDIBULAR SPACES -SUBMENTAL SPACE -BUCCAL SPACE -SUBMANDIBULAR SPACE -SUBLINGUAL SPACE
- 3. INTRODUCTION Infections of orofacial and neck regions range from periapical abscess to superficial and deep neck infections The infections spread by following the path of least resistance through connective tissue and fascial planes The infection spread to such an extent ,distant from the site of origin causing considerable morbidity and occasional death
- 4. PATHWAYS OF ODONTOGENIC INFECTIONS
- 5. Invasion of dental pulp by bacteria after decay of tooth -> Inflammation, edema, lack of collateral blood supply -> venous congestion or avascular necrosis ->Reservoir for bacterial growth ->periodic egress of bacteria into surrounding alveolar bone
- 6. SPREAD OF OROFACIAL INFECTIONS ROUTES OF SPREAD By direct continuity through the tissues By lymphatics to the regional lymph nodes and eventually into blood stream Which may lead to secondary areas of cellulitis or tissue space abscess By the blood stream If the infection remains confined to the peri-apical areas, chronic periapical infections develop , which leads to sufficient destructions of bone-> osteomyelitis
- 8. MAXILLA Swelling or fistula in the posterior part of hard palate it is related to palatal roots of molars Maxillary incisor and cuspid roots lie closer to thin labial plate of bone than to thicker palatal bone Infection from maxillary bicuspids may extend into connective tissue of buccal vestibule spread superiorly causing cellulitis of eyelids Infection from molars may exit from alveolar bone buccally, palatally or posteriorly Superior spread -> infratemporal space, maxillary sinus Posteriorly->masticator and pharyngeal space
- 10. MANDIBLE Infection of mandibular incisors and cuspids shows bulging in labial sulcus If infection spreads from bone deeper to origin of mentalis muscle->submental space Infection from mandibular 3rd molar involve buccal vestibule, buccal space, masticator space, parapharyngeal spaces
- 12. CLASSIFICATION OF FASCIAL SPACES BASED ON THE MODE OF INVOLVEMENT: Direct involvement:- Primary maxillary spaces- canine space, buccal space, infra temporal space Primary mandibular spaces- submental space buccal space, submandibular space, sublingual space Indirect involvement- Secondary fascial spaces- masseteric
- 13. Pterygomandibular space Superficial temporal space Deep temporal space Lateral pharyngeal space Retropharyngeal space Prevertebral space Parotid space Basedon clinical significance Face - Buccal , canine, masticatory, parotid Suprahyoid- sublingual, submandibular, pharyngomaxillary, peritonsillar Infrahyoid- anterovisceral(pre tracheal) Spaces of total neck: retropharyngeal , space of carotid sheath
- 14. The teeth which frequently give rise to abscess in this area are maxillary canines, premolars and sometimes mesiobuccal root of 1st molar
- 15. CANINE SPACE( INFRA-ORBITAL SPACE) Boundaries:- Anteriorly- orbicularis oris Posteriorly- buccinator Superiorly-levator labii superioris, zygomaticus minor Inferiorly- caninus muscle Medially- anterolateral surface of maxilla
- 16. CLINICAL FEATURES:- Swelling of cheek and upper lip Obliteration of nasolabial fold Drooping of the angle of mouth edema of lower eyelid Redness and marked tenderness of facial tissues Intraoral- offending tooth is mobile and tender on INCISION & DRAINAGE:- A curved mosquito forcep is inserted superior to the attachment of caninus muscle & the infra- orbital space is entered Pus is evacuated and a drain is inserted & secured to one of the margins with suture
- 18. It is the potential space between buccinator & masseter muscle Maxillary & Mandibular premolars and molars area involved. Location of the root tip to the level of origin of buccinator muscle determines the spread of infection either intraorally
- 19. Boundaries:- Anteromedially- buccinator muscle Posteromedially- masseter overlying the anterior border of ramus of mandible Laterally- forward extension of deep fascia from the capsule of parotid gland & platysma muscle Inferiorly- deep fascia to the mandible & depressor anguli oris Superiorly- zygomatic process of maxilla & zygomaticus major and minor
- 20. CLINICAL FEATURES:- Gum boil is seen in the vestibule (when the pus accumulates on oral side of the muscle) If the pus accumulates lateral to the muscle extraoral swelling is seen extending from lower border of mandible to the infra orbital margin and from anterior margin of masseter muscle to the corner of the mouth INCISION & DRAINAGE:- Horizontal incision through the oral mucosa of the cheek in the premolar molar region If the pus is lateral to the muscle then the muscle is penetrated with curved mosquito forceps to enter the buccal space Drain is placed secured with suture
- 21. It is also called “retrozygomatic space” The space is continuous with upper part of pterygomandibular space anteriorly, it is separated from it by lateral pterygoid muscle posteriorly The infratemporal fossa forms the upper extremity of pterygomandibular space
- 22. Involvement- Infections of the infratemporal space occurs from the infections of buccal roots maxillary 2nd and 3rd molars Local anesthesia injections with contaminated needles in the area of tuberosity Spread from other spaces infection Spread of infection Pus can extend upwards to involve the temporal space or inferiorly perforate the lateral pterygoid muscle to involve the pterygomandibular space It can spread through pterygoid plexus of veins upwards into cavernous sinus From infratemporal fossa to middle cranial fossa
- 23. Boundaries:- Laterally- ramus of mandible and temporalis muscle Medially-medial pterygoid plateand lateral pterygoid muscle superiorly - infratemporal surface of greater wing of sphenoid Inferiorly- lateral pterygoid muscle Anteriorly- infratemporal surface of maxilla Posteriorly -parotid gland
- 24. CLINICAL FEATURES:- Extraoral- trismus Bulging of temporalis muscle Marked swelling of the face on the affected side in front of the ear overlying area of tmj Intra oral –swelling in tuberosity area with elevation of temp 104F INCISION & DRAINAGE:- Intraoral approach- incision is given in buccal vestibule opposite 2nd and 3rd molar exploration is carried out medial to coronoid process and temporalis muscle upwards backwards with sinus forcep ,space is entered and drained Extra oral approach- incision is made at upper and posterior edge of temporalis muscle within hairline. Sinus forcep directed upward medially Pus is evacuated
- 26. Infections originating from 6 anterior mandibular teeth then perforate cortical plate below the origin of mentalis muscle labially ,mylohyoid lingually It can also affected from lower incisors , lower lip, skin overlying the chin, anterior part of floor of mouth, tip of tongue and sublingual tissues
- 27. BOUNDARIES:- Lateral- lower border of mandible and anterior bellies of digastric Superior:- mylohyoid muscle Inferior:- suprahyoid portion of the investing layer of deep cervical fascia
- 28. CLINICAL FEATURES:- Extraoral findings- distinct, firm swelling in midline beneath the chin Skin over the swelling is board like taut Intraoral findings- the anterior teeth are either non-vital fractured or carious . The offending tooth may exhibit tenderness to percussion may show mobility
- 29. Spread: of infection- Posteriorly- to involve submandibular space It may discharge on the face in the submental region INCISION & DRAINAGE:- A transverse incision is made in the skin below the symphysis of the mandible. Blunt dissection is carried out by inserting a kelly’s forcep through this incision ,upward ,backward Then corrugated rubber drain is inserted in the abscess cavity and sutured
- 30. The space lies between the anterior and posterior bellies of digastric muscle. Upper part lies beneath the inferior border of mandible and lower part lies deep to the investing layer of deep cervical fascia
- 31. INVOLVEMENT Infections originating from mandibular molars, pus perforates the lingual cortical plate of mandible passes directly into the submandibular space Infection from submental space Infection from posterior part of sublingual space Infections from middle third of the tongue, posterior part of floor of mouth, maxilary teeth,
- 32. BOUNDARIES:- Anteromedially:- floor is formed by mylohyoid muscle Posteromedially:- floor is formed by hyoglossus muscle superolaterally :- medial surface of mandible Anterosuperiorly:- anterior belly of digastric Posterosuperiorly:- posterior belly of digastric
- 33. CLINICAL FEATURES:- Extra oral:- firm swelling in the submandibular region, below inferior border of mandible Redness of overlying skin Intra oral:- teeth are sensitive to percussion Teeth are mobile Dysphagia Moderate trismus Spread: of infection- There is no major anatomic barriers so infection can extend into submental space There is no anatomical barrier so infection can spread easily across the midline involve submandibular space on other side It communicates with sublingual space around posterior border of mylohyoid muscle It can also spread into parapharyngeal space
- 34. An incision of about 1.5 to 2 cm length is made 2cm below the lower border of mandible Skin and subcutaneous tissues are incised Sinus forcep is inserted through the incision superiorly and posteriorly on the lingual side of mandible below the mylohyoid to release pus from submandibular space INCISION & DRAINAGE:-
- 35. Space is a “V” shaped trough lying lateral to muscles of tongue including hyouglossus, genioglossus, geniohyoid Involvement:- mandibular incisors, canines, premolars , sometimes molars It is a paired space but the 2 sides communicates anteriorly, with submandibular space around the posterior border of mylohyoid muscle
- 36. BOUNDARIES:- Inferiorly- mylohyoid muscle Laterally:- medial side of the mandible above mylohyoid muscle Medially:- hyoglossus, genioglossus & geniohyoid muscles Posteriorly:- hyoid bone Laterally and inferiorly:- mylohyoid muscle and lingual side of mandible
- 37. CLINICAL FEATURES:- Extraorally: there is little or no swelling. The lymph nodes may be tender & enlarged Pain and discomfort on deglutition Intraorally: firm, painful swelling seen in the floor of the mouth Floor of the mouth is raised Tongue pushed superiorly will cause airway obstruction Spread: of infection- Infection crosses the midline and effect the space on the opposite Infection from posterior inferior part of the space spread into submandibular space-> pterygomandibular and parapharyngeal space Infection spread via lymphatics to the submandibular or submental lymph node
- 38. INCISION & DRAINAGE:- Inraorally:- incision is made close to the lingual cortical plate, lateral to sublingual plica (whartons duct, sublingual artery,veins & lingual nerve) Sinus forceps is then inserted and openeed to evacuate the pus Extraorally:- when both submental and sublingual space contains pus they can be drained by placing incision in submental region
- 39. MANAGEMENT OF OROFACIAL INFECTIONS Antibiotic therapy:- Use of penicillin G (2 to 4 million units, IV 4 to 6 hrs)and metronidazole(400 mg 8 hourly orally or IV) Oral clindamycin Amoxicillin-clavulanic acid(augmentin) 1st and 2nd generation cephalosporins are useful in orofacial infections In compromised patients- clindamycin alone 300 to 600 mg 8 hourly IV) Or in combination with gentamycin ( 80 mg IM) can be given SURGICAL THERAPY Hilton’s method of incision and drainage The method of opening an abscess ensures that no blood vessels or nerve is damaged Incision helps to get rid of toxic purulent material To allow better perfusion of blood containing antibiotic and defensive elements To increase oxygenation of infected area
- 40. HILTON’S METHOD OF INCISION AND DRAINAGE Topical anesthesia:- achieved with the help of ethyl chloride spray Stab incision:- it is made over the point of maximum fluctuation in the most dependent area through skin and subcutaneous tissue Deepening of surgical site is achieved with sinus forceps Closed forceps are pushed through deep fascia move towards the pus collection
- 41. Abscess cavity is entered and forceps is opened in a direction parallel to vital structures Pus flow along side of beaks Explore the entire cavity for additional loculi Placement of drain:- A corrugated rubber drain is inserted into depth of abscess cavity & external part secured with suture Drain is left for 24 hrs Dressing:- applied over the site of incision taken extraorally without pressure
- 42. INVOLVEMENT OF MULTIPLE PRIMARY SPACES LUDWIG’S ANGINA It is a firm, massive, brawny cellulitis and acute, toxic stage involving simultaneously submandibular, sublingual, submental space bilaterally It means “suffocation or choking sensation” Clinical features:- There is pyrexia, anorexia , chills, malaise Severe muscle spasm may lead to trismus with restricted mouth opening and also jaw movements Tongue movements may be reduced Air obstruction Fatal death may occur in untreated case of Ludwig’s angina within 10 to 24 hours due to asphyxia
- 43. TREATMENT OF LUDWIG’S ANGINA Early diagnosis Maintenance of the patient airway Intense and prolonged antibiotic therapy Extraction of offending teeth Surgical drainage or decompression of fascial spaces
- 44. THANK YOU