3. ∏ Area between a superior plane drawn through the FZ sutures
tangential to the skull base and inferior plane at the level of
maxillary occlusal surface
∏ Triangular region with widest dimension facing anterior
4. ∏ Middle 3rd of face is composed of
Paired Bones Unpaired Bones
Maxilla Vomer
Zygomatic bone Ethmoid
Zygomatic process of
temporal bone
Sphenoid (Pterygoid plates)
Palatine bone
Nasal bone
Lacrimal bone
Inferior conchae
5. ∏ Maxilla –central bone; prominent
position where trauma hits face
∏ This structure is analogous to a
matchbox sitting below and anterior
to hard shell containing brain
∏ Act as cushion for trauma directed
towards cranium from anterior or
antero-lateral direction
6. ∆ Areas of weakness act as “crumple zone”.
∆ Sutures
∆Areas of strength: pillars of face
7. ∏ This arrangement with stands force of mastication
from below and protects the vital structure
∏ Bones easily fractured from forces applied from
other directions.
∏ Clinical implications
9. 1. Alphonso Guerin(1886)
2. Rene Le Fort Fracture classification (1901)
3. Rowe and william classification (1985)
4. Modified Le fort classification (Marciani,1993)
5. Donag,Endress,Mathog classification(1998)
10.
11. Pitfalls:
a) # caused by loc penetrating missile injuries & gun
shot wounds not
included.
b) Only meant for bilateral # occuring at same level
c) mid palatine split along palatal suture not described
d) Inaccurate prediction of reduction techniques.
12. Fracture not involving the occlusion
Central region
Nasal bone/ septum (lateral, anterior injuries)
Frontal process of the maxilla
Nasoethmoid
Fronto-orbito-nasal dislocation
Lateral region (zygomatic complex ,arch, dento-alveolar fracture
Fracture involving the occlusion
Dento alveolar
Subzygomatic:
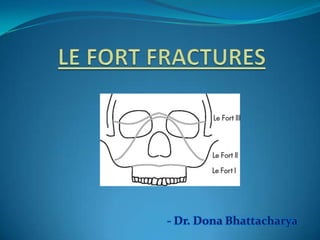
Le Fort (I, II)
Supra zygomatic:
Le Fort III
13.
14. From: Donat TL et al. Facial Fracture Classification According to Skeletal Support
Mechanisms. Arch Otolaryngol Head Neck Surg 1998;124:1306-1314.
16. Prevalence of mid-face
fractures
Fracture Type Prevalence
Zygomaticomaxillary complex (tripod fracture) 40 %
LeFort
I 15 %
II 10 %
III 10 %
Zygomatic arch 10 %
Alveolar process of maxilla 5 %
Smash fractures 5 %
Other 5 %
17. A). Le fort I/ Floating fracture/ Guerin fracture/ Low level
fracture/ Subzygomatic fracture
1. Mobility of maxillary alveolar segment (floating fracture)
2. Pain and tenderness while speaking or clenching
3. Ecchymosis or laceration in labial or buccal vestibule
4. Ecchymosis at GP foramen (Guerin sign)
5. Swelling and oedema of upper lip
6. Mal occlusion
7. Bilateral epistaxis
8. Brusing of palatal tissues (15-20% of cases)
9. On palpation tenderness over buttress area
10. Percussion of teeth – cracked pot sound
Clinical Features
18. B). Le fort II/ Pyramidal fracture/ Mid level fracture/ Subzygomatic
fracture
1. Oedema mid third of face (Moon face)
2. Paresthesia of cheek
3. Bilateral circumorbital ecchymosis
4. Bilateral subconjunctival haemorrhage
5. Dish face deformity
6. Depressed nose
7. Epistaxis
8. CSF rhinorrhea
9. Limited ocular movement (Diplopia)
10. Mal occlusion
11. Inability to open mouth
12. Step deformity at IO margins
13. Mobility of fractured fragment at nasal bridge and IO margins
14. Percussion of teeth – cracked pot sound
19. C). Le fort III/ Craniofacial dysfunction/ High level fracture/
Suprazygomatic fracture
1. Oedema of face (Panda facies)
2. Bilateral periorbital edema
3. Bilateral circumorbital ecchymosis (Racoon eyes)
4. Bilateral subconjunctival haemorrhage
5. Dish face deformity
6. Depressed nose, flattening of nose
7. Epistaxis
8. CSF rhinorrhea
9. Limited ocular movement (Diplopia, Enophthalmos)
10. Dystopia, hooding of eyes with antimongloid slant
11. Haemotympanum
12. CSF otorrhoea
13. Mal occlusion – posterior gagging of occlusion
14. Inability to open mouth
15. Mobility of fractured fragment at NF, FZ sutures
16. Tenderness over zygomatic bone, arch and FZ suture
17. Ecchymosis at mastoid process (Battle’s sign)
20. 1. Emergency care and stabilization
2. Initial assessment
3. Definitive treatment
4. Continuing care
21. ∆ Airway immediately evaluated for obstruction
∆Control of oral or nasal bleeding
Possibility of C – spine fracture – endotracheal incubation
should not be attempted
Cervical collar in case of suspected spine fractures
∆Circulation
22. LeFort I fracture
LeFort I fracture with Mandible fracture
LeFort I fracture with Nasal injury
LeFort II fracture
Lefort III fracture
Panfacial fractures
Nasal Airway
Edentulous Partially Dentate
with space
Fully Dentate
Oral Airway
through portal
cut in Gunning
splints or
dentures
Oral Airway
with tube
displaced
through space
Surgical
Airway
Guided Nasal
Intubation
• fixate maxilla
and mandible
• switch to Oral
Airway for
nasal/NOE
reduction
23. Premlatha Shetty et al;submental intubation in patients with panfacial fractures;Indian journal of anesthesia,vol
55,issue 3,may 2011
24. 1. History
2. Palpation of entire facial skeleton
3. I/O Examination
4. Ophthalmologic exam / consultation
5. Radiographic examination
25. After stabilization of patients condition, complete facial
examination is performed.
1. Laceration, bruising , etc.
2. Obvious depressions on nose, check, etc.
3. Facial asymmetry, swelling
4. Nasal discharge (Blood/ CSF)
26. Features CSF fluid Nasal secretion
History Nasal or sinus surgery, head injury or
intracranial tumour
Sneezing, nasal stuffiness,
itching in the nose or
lacrimation
Flow of discharge A few drops or a stream of fluid gushes
down when bending forward or
straining; can’t be sniffed back
Continuous. No effect of
bending forward or
straining. Can be sniffed
back
Character of
discharge
Thin, watery and clear Slimy (mucus) or clear
(tears)
Taste Sweet Salty
Sugar content More than 30 mg/dl (Compare with
sugar in CSF after lumbar puncture as
sugar is less in CSF in meningitis)
Less than 10 mg/dl
Presence of β2
transferrin
Always present. It is specific for CSF Always absent
31. 1. OPG
2. OM
3. Lateral skull view
4. Occlusal view for split palate
5. CT Scan
6. 3D CT Scan
7. MRI
32. ∆ Aims of treatment
1. Relieve pain
2. Precise anatomical reduction of the # fragment
3. Stable fixation of the reduced fragment
4. Restore function
5. Restore the dental occlusion
33. Preoperative planning:
∆ Need for surgical airway
∆ Open/closed method of reduction
∆ Necessity for and type if IMF to be employed in case for
closed reduction
∆ Type of osteosynthesis in case of open method
∆ Need for internal suspension in case of communited #
∆ Timing of surgery
34. ∏ Optimum time for reduction of mid face fracture is 5th to 8th
post injury day
∏ After this with every succeeding day disimpaction become
difficult and open reduction more essential
35. Open reduction Closed reduction
Displaced # Non displaced #
Multiple # of facial bones Grossly communited #
Edentulous maxillary # - with severe
displacement
Fractures associated with significant
loss of soft tissues
Edentulous maxillary # - opposite to
Edentulous mandibular #
Edentulous maxillary #
Delay of treatment In children with developing dentition
Inter position of soft tissues between
non contacting displaced # segment
Systemic condition contra indicating
IMF
36. 1. Accurate diagnosis
2. Determination of priority of treatment
3. Early reconstruction
4. Wide exposure of vertical and horizontal pillar of face
5. Use of bone graft to restore skeletal form
6. Use of rigid fixation to stabilize # segment
7. Restoration of bony support to over lying soft tissue envelop
37. 1. Intra oral
a) Vestibular
2. Extra oral
a) Lower eye lid incision
i. Sub cilliary
ii. Infra orbital
iii. Trans conjunctival
b) Coronal approach
c) Midface degloving approach
45. 1. Manual reduction
2. Reduction with wires
3. Reduction using disimpaction
forceps
4. Reduction with bone hook
5. Reduction with elastics
46. 1. Simple manipulation by hand
2. Use of dental compound loaded in impression tray
(Dingman and Harding, 1951)
3. Use of rubber dam sheets, long ribbon/strip gauze or
rubber catheter (Propescu and Burlibasa, 1966)
48. Movements:
1. Downwards – to affect disimpaction
of pterygoid plates down
2. Anterior
3. Combination of forward traction
with rotational movement in both
horizontal and vertical axis
Universal rule
Oculocardiac reflex
49. Used in delayed cases:
1. Intra oral elastic traction
2. Extra oral elastic traction
53. Miniplates and screws
These are monocortical, semi-rigid fixation device which
provide 3D stability.
Designs: X, H, L, T, Y
Thickness:0.6-1 mm
54. Plating system depends on:
1. Rigidity of plate
2. Width and shape
3. Diameter and number of screws
Increase in width provides more stability towards rotational forces.
Type of metal:
a. Stainless steel
b. Titanium
c. Vitallium
Advantages:
1) Easily adaptable
2) Monocortical
3) Functional stability
4) Reduced surgical access
55. 1. Minimum 2 screws required in each bone segment to prevent
rotation in X and Y axis
2. Farther the point of stabilization the more effective the device
is in preventing rotation
3. Large diameter screws are not used because of constraint
imposed by particular anatomic location
4. All screw require adequate intervening bone between adjacent
holes to preserve integrity of screw bone interface
56. Le fort I: L plates at zygomatic buttress
Curved plate at pyriform aperture
3D plate sometimes to fix buttress #
Le fort II: Linear/Y plate/curved plate along intra orbital rim
L plate at buttress
Le fort III: Linear/Y plate at FN and ZF junction
57. Harle & duker(1975;Luhr(1979)
0.3-0.6 mm
Used for :
a. FN region
b. Frontal bone
c. Frontal process of maxilla
Sites of application:
a. Linear/T/Y plate at FN region
b. Long curve plate for frontal process of maxilla or frontal bone
58. Used for retention and alignment
of small fragments or bone
grafts.
Sites of application:
1. Anterior and lateral wall of
maxilla
2. Anterior table of frontal bone
59.
60. Introduced by Kuffner, 1970
Two types
1. Central
2. Lateral
Usually used for high midface
fracture.
61. Incision in lateral 3rd/nasal process of
frontal bone
Exposure of zygomatic proces/outer
cortex of frontal bone
Drilling of bur hole and placement of
screw
Passage of SS wire attached to awl;
through incision into maxillary
vestibule
Release of wire and attachment to the
arch bar
62. Indication: le fort II and III fracture
Incision in maxillary vestibule above
canine
Subperiosteal dissection and
exposure of infra orbital rim
Drill hole and passage of wire above
IO rim and back to oral cavity
Release of wire and attachment to
the arch bar
63. Also known as buttress wire
Incision in maxillary vestibule below buttress
Exposure of ZM junction
Drill hole and passage of wire
Release of wire and attachment to the arch bar
65. Introduced by Bowerman and
Conroy, 1981
Simple technique for fixing
gunning splint to maxilla
Superior retention, stability and
decreased discomfort
Incision in maxillary vestibule over nasal
spine
Exposure of ANS
Drill hole and passage of wire
Release of wire and attachment to the arch
bar
66. Incision in maxillary vestibule in canine fossa
Subperiosteal dissection and exposure of
pyriform aperture
Elevation of nasal mucosa and drill hole from
lateral to medial
Passage of wire and attachment to the arch
bar
67. Drill hole in palatal aspect of splint
Direct wire through alveolus over canine region and
emerge in Buccal Sulcus
Passage of 0.5 mm SS wire and secure to splint
68. Trend towards ORIF has changed
External fixation is used in cases where there is depressed posterior
displaced #
Principle:
External appliances relies on sandwiching the midface between base of
skull and mandible to provide cantilever support to midface in 3D
following disimpaction and closed reduction.
Disadvantages:
70. Described by Crawford;modified by
Mackenzie & Ray,1970
Secure the frame work to the skull
directly by screw pins
Advantage:
1. Light weight
2. Adjustable
3. Titanium Screw pin
71. ∏ More stable and rigid
∏ Other unstable fracture fragment
can also be attached to vertical rod
72. ∏ Developed at Royal
Melbourne Hospital
∏ Provided simple rigid
craniomaxillary
fixation between
supraorbital rims and
maxilla connected by
central rod attached
at lower end by means
of cast metal splint or
acrylic splint
73. 1. Provide dimensional stability
2. Indications:
1. Grossly communited #
2. Extensive soft tissue loss
3. Bone gap>5mm
3. Sites:
1. Calvarium
2. Illium
3. Rib
75. Immediate
1. Airway
2. Nasal hemorrhage
3. Ophthalmic complications
4. Inaccurate reduction
5. Insecure fixation
Late complications
1. Non union
2. mal occlusion
3. Cranial nerve dysfunction
4. Secondary nasal deformity
5. Dacrocystitis
6. Facial asymmetry
76. Due to the complex 3D arrangement of the structures of middle
third of face,management is complicated.Proper reduction of
the # fragments remains the key component.
A proper understanding of the anatomy,fracture patterns, its
clinical presentation and the available treatment modalities is
necessary to successfully treat Le Fort Fractures.
77. 1. Oral & maxillofacial trauma-Fonseca & walker vol 2
2. Oral & maxillofacial surgery-Fonseca vol 3
3. Oral & maxillofacial trauma-Rowe & Williams vol 2
4. Principles of Oral & maxillofacial surgery-Peterson
5. Fractures of middle third of face-Killey & Kay
6. Oral & maxillofacial surgery-Fragiskos
7. Maxillofacial trauma & facial reconstruction-Peter Ward Booth
8. Oral & maxillofacial surgery-Peter Ward Booth: vol 2
9. Chen Lee et al ;Applications of the Endoscope in Facial fracture
Management, seminars in plastics surgery/volume 22, number 1
2008
78. 9. Manual of internal fixation-J Prein
10. Donat TL et al. Facial Fracture Classification According to Skeletal
Support Mechanisms. Arch Otolaryngol Head Neck Surg
1998;124:1306-1314.
11. Mirko S. Gilardino et al;Choice of Internal Rigid Fixation
materials in the treatment of facial fractures; craniomaxillofacial
trauma & reconstruction/volume 2, number 1 2009
12. Khaled M Emara et al ;Methods to shorten the duration of an
external fixator in the management of fractures; World J Orthop
2011 September 18; 2(9): 85-92
13. Chan hum park et al;resorbable skeletal fixation systems for
treating maxillofacial bone fractures; arch otolaryngol head neck
surg/vol 137 (no. 2), feb 2011
14. Premlatha Shetty et al;submental intubation in patients with
panfacial fractures;Indian journal of anesthesia,vol 55,issue 3,may
2011.