
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (11)
Similar to Rosacea: Inflammatory condition in Dermatology
Similar to Rosacea: Inflammatory condition in Dermatology (20)
Recently uploaded
Recently uploaded (20)
Rosacea: Inflammatory condition in Dermatology
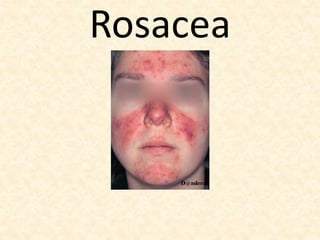
- 1. Rosacea
- 2. Objectives: • Introduction and classification of Rosacea • Epidemiology • Pathophysiology • Clinical features • Differential Diagnosis • Treatment of Rosacea.
- 3. Definition: It is a chronic disorder affecting the facial convexities characterized: • Frequent flushing • Persistent erythema • Telangiectasias, • Interspersed by episodes of inflammation characterized by swelling, papules and pustules.
- 4. Classification and Grading of Severity: Classification: 1.Subtype 1:Erythematotelangiectatic Rosacea (ETTR) 2.Subtype2:Papulopustular Rosacea (PPR) 3.Subtype 3:Phymatous Rosacea (PR) 4.Subtype 4:Ocular Rosacea (OR)
- 5. Grading: Grade 1: Mild disease Grade 2: Moderate disease Grade 3: Severe disease
- 6. Epidemiology: • Disease of the fair-skinned, sun sensitive individuals • Males and females equally affected. • Males affected with more severe rosacea and with rhinophyma • Peak age of incidence in 30-40 years. • Subtype 1 (ETTR) is by far the commonest type.
- 7. Pathophysiology: 1. Genetic Factors: 25% patients have a family history 2.Ultraviolet Radiation and Adverse weather conditions: (a) Photo-exposed areas (b) Condition is exacerbated by wind
- 8. 3.Causative Organisms: (a) Demodex Mite (b) Staphylococcus epidermidis (c) Chlamydophilia pnuemoniae (d) Bacillus Oleronius 4. Alteration in Cutaneous Microenvironment (a) Changes in cutaneous pH (b) Alteration in the skin barrier function (c) Changes in lipid profile
- 9. 5.Meibomian Gland dysfunction: (a) Reduced tear break up time (b) Demodex mite infestation 6. Environmental Factors: (a) Increased ambient temperature (b) Ingestion of hot liquids, spicy foods & large meals (c) Alcohol consumption
- 10. Pathogenesis: Altered Innate Immune response leads to the following: (a)Increased Toll like receptor 2 activity (b)Increased protease activity and cathelicidin production. (c) Leukocyte chemotaxsis (d) Increased angiogenesis (e) Extracellular matrix production.
- 12. Histopathology of ETTR: 1.Enlarged bizarre shaped capillaries and venules in upper part of dermis 2.Mild perivascular and interstial infiltrate of lymphocytes and plasma cells 3.Occasionally demodex mites 4.Solar elastosis
- 13. Histopathology of Papulopustular Rosacea: • Dense follicular and perivascular infiltrate of lymphocytes, plasma cells, neutrophils, and mast cells.
- 14. Histopathology of Rhinophyma • Sebaceous gland Hyperplasia • Striking dermal fibrotic changes • Variable degree of perivascular lymphocytic/neutrophilic infiltrate. • Demodex mites
- 15. Histopathology of Ocular Rosacea: Posterior meibomian glands are affected with lymphocytic, histiocytic and neutrophilic infiltrate
- 16. Clinical Features: 1)Erythematotelangiectatic Rosacea: • Gradual increase in facial redness. • Episodes of flushing in response to environmental changes and food • Appearance of telangiectasia (broken blood vessels) • Increased sensitivity of the skin to topical applications • Evidence of solar damage (actinic keratoses, actinic lentigines)
- 18. 2.Papulopustular Rosacea (PPR): • Appearance of papules and pustules. • Prominent perilesional erythema • Larger pustules but all lesions are superficial • NODULES AND CYSTS ARE NOT A FEATURE OF PPR • Lesions at different stages of evolution • Heal without scarring or leave persistent post-inflammatory erythema.
- 20. 3.Phymatous Posacea (PR): • Includes: Rhinophyma Otophyma (Enlarged ears) Metophyma (Thickening of the skin of the forehead) • Rhinophyma – the commonest form of PR and seen mostly in males • Thickening of skin of distal nose. • Prominent follicular openings. • Distal end of the nose becomes bulbous and greasy.
- 21. Rhinophyma has also been called copper nose, brandy nose or bulbous nose
- 22. 4.Ocular Rosacea: • Sensation of grittiness and dryness • Watery eyes • Blephritis • Stye formation • Chalazion • Conjunctival hyperemia and fibrosis • Photophobia and blurred vision • Keratitis
- 24. Clinical Variants: Granulomatous Rosacea: 1.Persistent , firm, non tender red to brown papules on normal skin. 2.Sites: around the mouth, eyes and cheeks 3.Monomorphic picture 4.Treatment resistant and heals with significant scarring 5.Histopathology: granulomatous change with foci of caseation necrosis.
- 25. Differential Diagnosis: Erythematotelangiectatic Rosacea: 1.Chronic photodamage 2.Seborrhoeic Dermatitis 3.Lupus erythematosus 4.Contact dermatitis of face 5.Ulerythema ophyrogenes
- 26. Papulopustular Rosacea: 1. Acne vulgaris 2. Rosacea like dermatoses 3. Pityriasis folliculorum 4. Perioral dermatitis 5. Jessner’s lymphocytic infiltrate 6. Tinea facei
- 27. Phymatous Rosacea: 1.Lupus pernio 2.Granuloma faciale 3.Lymphocytoma cutis 4.Solid facial lymphedema 5.Basal cell carcinoma, squamous cell carcinoma and lymphomas. Ocular Rosacea: Other causes of blepharitis.
- 28. Complications and Co-morbidities: • Increased risk of cardiovascular disease • OR leads to visual impairment through recurrent episodes of keratitis. • Basal cell carcinoma may be obscured by phymatous tissue. • Seborrheic dermatitis may co-exist with roscea. • Lymphedema affecting any part of the face and ears leading to coarse features and leonine facies
- 29. Disease Course and Prognosis: Chronic condition with relapses and remissions. ETTR: Skin becomes increasingly sensitive and flushing more frequent. PPR: Lesions heal with perilesional erythema contibuting to overall erythema of face Rhinophyma: Progresses from nose enlargement to distortion. OR: progresses to conjunctival fibrosis, punctate keratitis and corneal revascularization