Electrophysiology study protocol
•Download as PPTX, PDF•
38 likes•5,479 views

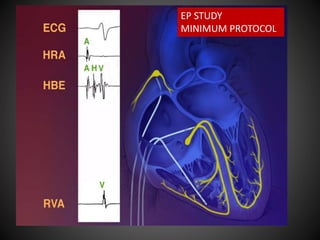
Minimum protocol for Electrophysiology study of conduction in heart.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Electrophysiology study protocol
Similar to Electrophysiology study protocol (20)
More from Satyam Rajvanshi
More from Satyam Rajvanshi (7)
Recently uploaded
Recently uploaded (20)
Electrophysiology study protocol
- 2. WE’VE TALKED ABOUT… EQUIPMENT PATIENT PREPARATION RELEVANT ANATOMY CATHETERS and PLACEMENT BASIC INTERVALS TESTS OF SN FUNCTION
- 3. AND NOW… EQUIPMENT PATIENT PREPARATION RELEVANT ANATOMY CATHETERS and PLACEMENT BASIC INTERVALS TESTS OF SN FUNCTION ATRIAL and VENTRICULAR EXTRASTIMULUS TESTING REFRACTORY PERIODS ‘GAP’ INCREMENTAL PACING MINIMUM PROTOCOL FOR DIAGNOSTIC EPS
- 5. 5 Drive train with a single extra stimulus S1 S1 S1 S1 S1 S1 S1 S1 S2Sensed PAUSEDRIVETRAIN S1-S2 Interval Sense-S1 Interval 8 paced beat drive train – EP steady state Extrastimulus (Coupling interval)
- 6. Extra stimuli S 1 S 1 S 1 S 1 S 1 S 1 S 1 S 1 S 2Sensed DRIVETRAIN S 3 S 4 S1 S1 S1 S1 S1 S1 S1 S1 S2Sensed DRIVETRAIN S 1 S 1 S 1 S 1 S 1 S 1 S 1 S 1 S2Sensed DRIVETRAIN S3 Single Double Triple
- 7. Atrial Extrastimulus testing • Dynamic properties of AVN and HPS conduction • AVN and RA refractory periods
- 8. Atrial Extrastimulus testing • Dynamic properties of AVN and HPS conduction • AVN and RA refractory periods • Dual AVN physiology
- 9. Atrial Extrastimulus testing • Dynamic properties of AVN and HPS conduction • AVN and RA refractory periods • Dual AVN physiology • Arrhythmia induction
- 10. S2 with long coupling interval Conduction at fairly constant velocity A2H2 equal or slightly more than A1H1
- 11. A1H1 80 ms ~ A2H2 95 ms S1A1 ~ S2A2 ~ 55 ms H1V1 ~ H2V2 ~ 50 ms
- 12. S2 with short coupling interval Slowing of Conduction A1H1 < A2H2
- 13. A1H1 80 ms A2H2 140 ms
- 14. S2 with shorter coupling interval Blocked AES at AVN
- 16. Ventricular Extrastimulus testing • Retrograde conduction over HPS and AVN • Accessory pathway conduction • Arrhythmia induction
- 17. Ventricular Extrastimulus testing • Retrograde conduction over HPS and AVN • Accessory pathway conduction • Arrhythmia induction • Stimulation at RV apex conventionally – RV apex Stim – distal RBB – HPS – AVN – RA
- 18. S2 with long coupling interval
- 19. H buried in V V1A1 almost equal to V2A2 Earliest atrial activation in HBE Atleast 30 ms before HRA Proximal-to-distal CS activation CONCENTRIC ATRIAL ACTIVATION
- 20. S2 with short coupling interval
- 21. S2 with shorter coupling interval
- 22. S2 with short coupling interval with short drive cycle length Blocked VES at AVN VA block Differs with – ES coupling interval – Drive cycle length
- 23. S2 with short coupling interval Tissue latency in local evoked response Occurs just above the tissue refractory period
- 24. Even shorter coupling interval Blocked VES locally at RV apex Loss of ventricular capture
- 25. Ventricular Extrastimulus testing • Other ‘Normal’ responses – No VA conduction at all • Atropine, Isoprenaline • No VA conduction despite drugs
- 26. Ventricular Extrastimulus testing • Other ‘Normal’ responses – No VA conduction at all • Atropine, Isoprenaline • No VA conduction despite drugs – Retrograde exit site from AV node maybe near CS ostium rather than HBE – earliest atrial activation at Proximal CS
- 27. Ventricular Extrastimulus testing • Other ‘Normal’ responses – No VA conduction at all • Atropine, Isoprenaline • No VA conduction despite drugs – Retrograde exit site from AV node maybe near CS ostium rather than HBE – earliest atrial activation at Proximal CS • Maneuvers to prove accessory pathway
- 29. EFFECTIVE Refractory Period • ERP of a tissue
- 30. EFFECTIVE Refractory Period • ERP of a tissue (or a structure)
- 31. EFFECTIVE Refractory Period • ERP of a tissue (or a structure) is the LONGEST coupling interval that fails to capture the tissue
- 32. EFFECTIVE Refractory Period • ERP of a tissue (or a structure) is the LONGEST coupling interval that fails to capture the tissue (or be conducted over the structure)
- 33. FUNCTIONAL Refractory Period • FRP of a tissue (or a structure) is the SHORTEST ‘output’ coupling interval that can be elicited from a tissue (or structure) by any ‘input’ interval
- 34. FUNCTIONAL Refractory Period • FRP of a tissue (or a structure) is the SHORTEST ‘output’ coupling interval that can be elicited from a tissue (or structure) by any ‘input’ interval S1-A1-H1-V1 S2-A2-H2-V2 AVN HPS AV conduction system
- 35. RELATIVE Refractory Period • RRP of a tissue (or a structure) is the ‘input’ interval at which the ‘output’ interval just begins to differ from ‘input’ interval
- 36. RELATIVE Refractory Period • RRP of a tissue (or a structure) is the ‘input’ interval at which the ‘output’ interval just begins to differ from ‘input’ interval • This is the point at which Latency or Decremental conduction begins to occur • Least commonly measured
- 37. • In all tissues, ERP and FRP are ‘length- dependent’ • So, measured using atleast 2 different drive cycle lengths
- 38. AVNERP Longest A1A2 interval that fails to capture HB A1A2 maybe longer than S1S2 due to tissue latency
- 39. AVNFRP Shortest H1H2 in response to any A1A2 interval
- 40. AVNRRP Longest A1A2 interval at which A2H2 exceeds A1H1
- 42. Normal range of refractory periods (ms) ERP Atria ERP AVN FRP AVN ERP HPS ERP V 150-350 230-430 330-530 330-450 190-290 *Denes, Akhtar, Durrer, Josephsen series
- 49. MINIMUM PROTOCOL • Basic intervals • SNRT and CSNRT • AES – AVNERP • AV WCL • VES – VERP • VA WCL
- 52. ….NEXT presentations • Atrial arrhythmias • Ventricular Pre-excitation and AVRT • Ventricular arrhythmias • Catheter ablation