Absence Seizures .. Dr Padmesh
•Download as PPTX, PDF•
29 likes•18,655 views

Absence Seizures in Children

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (18)
Similar to Absence Seizures .. Dr Padmesh
Similar to Absence Seizures .. Dr Padmesh (20)
More from Dr Padmesh Vadakepat
More from Dr Padmesh Vadakepat (16)
Recently uploaded
Recently uploaded (20)
Absence Seizures .. Dr Padmesh
- 2. • Typical absence seizures have a bimodal distribution for age of onset; • First peak at 5-8 years (childhood) • Second peak near 12 years of age (juvenile)
- 3. • Childhood Absence Epilepsy (CAE) • CAE is a childhood epilepsy syndrome occurring in 10–17% of all childhood onset epilepsy. • The most common pediatric epilepsy syndrome. • Females > males
- 4. • Usually start at 5-8 yr of age. • No aura. • Usually last for only a few seconds.
- 5. • Accompanied by eye lid flutter or upward rolling of eyes. • Absence seizures can have simple automatisms like lip-smacking or picking at clothing. • Head can minimally fall forward. • No postictal period.
- 6. • Hyperventilation for 3-5 min can precipitate the seizures and the accompanying 3 Hz spike–and– slow-wave discharges.
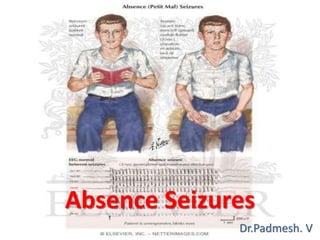
- 7. • EEG: • The ictal EEG of a typical absence seizure demonstrates: • generalized spike and wave complexes • that are > 2.5 Hz, typically 3–4.5 Hz , and • lasting ≥ 3 seconds. 3/sec spike-and-wave discharge of absence seizures with normal background activity
- 8. • The presence of periorbital, lid, perioral or limb myoclonic jerks with the typical absence seizures usually predicts difficulty in controlling the seizures with medications.
- 9. • Early onset absence seizures (before 4 yr) Evaluate glucose transporter defect that is often associated with low CSF glucose levels and an abnormal sequencing test of the transporter gene.
- 10. • Atypical absence seizures : • Associated myoclonic components. • Tone changes of the head (head drop) and body. • Variable impairments of consciousness. • Last longer than typical absences. • Precipitated by drowsiness. • Not provoked by hyperventilation or photic stimulation. • Usually more difficult to treat. • 1-2 Hz spike–and–slow-wave discharges.
- 11. • Juvenile absence seizures: • Similar to typical absences. • But occur at a later age. (10-17 years) • Accompanied by 4-6 Hz spike–and–slowwave and polyspike–and–slow-wave discharges. • Usually associated with juvenile myoclonic epilepsy
- 12. • TREATMENT: • Initial treatment: Ethosuximide (less toxic than valproate and more effective than lamotrigine.) • Alternative drugs of first choice are lamotrigine and valproate, especially if generalized tonic–clonic seizures coexist with absence seizures. (as these 2 medications are effective against the latter seizures whereas ethosuximide is not.) • EEG often normalizes when complete seizure control is achieved.
- 13. • TREATMENT: • Other medications that could be used for absence seizures include – Acetazolamide, – Zonisamide, or – Clonazepam.
- 14. • Outcome and Prognosis of Childhood Absence Epilepsy • Remission rates : 21%–74% • Although labeled “benign”, the clinical course of CAE is variable and remission rates are far lower than in other classic benign idiopathic epilepsies such as Benign Rolandic Epilepsy. • Multiple studies report that GTCs ultimately develop in roughly 40% of children with absence seizures at onset.
- 15. • Outcome and Prognosis of Childhood Absence Epilepsy • GTCs often occur 5 to 10 years after the onset of the absence seizures between 8–15 years old. • Risk factors include: – Onset of absence seizures after 8 years old, – Male sex, – Lack of response to initial therapy and – Therapy with only an anti-absence drug. • Accidental injury is common.