Respiratory Disorders
Disease Condition Pneumothorax, Causes, Sign and Symptoms, Pathophysiology, Types, Assessment and Dignostic Test, Management
By HIREN GEHLOTH For Nursing Students Medical Surgical Nursing
LAUGH A LOT IT CLEARS THE LUNGS
TEACHING IS ONE PROFESSION THAT CREATE ALL OTHER PROFESSION
3. INTRODUCATION
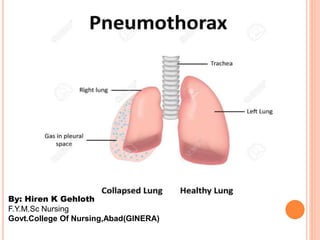
Pneumothorax is defined as
the presence of air or gas in
the pleural cavity (ie, the
potential space between the
visceral and parietal pleura
of the lung), which can
impair oxygenation and/or
ventilation. The clinical
results are dependent on the
degree of collapse of the
lung on the affected side.
4. If the pneumothorax is
significant, it can cause a
shift of the mediastinum
and compromise
hemodynamic stability.
Air can enter the
intrapleural space through
a communication from
the chest wall (ie, trauma)
or through the lung
parenchyma across the
visceral pleura.
5. DEFINITION
A pneumothorax is the presence of air between the
two layers of pleura (thin, transparent, two-
layered membrane that covers the lungs and also
lines the inside of the chest wall), resulting in
partial or complete collapse of the lung.
7. 1. SIMPLE PNEUMOTHORAX
A Simple, or spontaneous, pneumothorax occurs
when air enters the pleural space through a breach
of either the parietal or visceral pleura.
Most, commonly, this occurs as air enters the
pleural space through the rupture of a bleb or a
bronchopleural fistula.
A spontaneous pneumothorax may occur in an
apparently healthy person in the absence of trauma
due to rupture of an air filled bleb, or blister, on the
surface of the lung, allowing air from the airways to
enter the pleural cavity.
8. It may be associated with diffuse interstitial lung
disease and sever emphysema.
9. Primary Spontaneous:
Primary spontaneous pneumothorax (PSP) occurs in
people without underlying lung disease and in the
absence of an inciting event.
In other words, air enters into the intrapleural space
without preceding trauma and without an underlying
history of clinical lung disease.
However, many patients whose condition is labelled
as primary spontaneous pneumothorax have
subclinical lung disease, such as pleural blebs, that
can be detected by CT scanning.
Patients are typically aged 18-40 years, tall, thin,
and, often, are smokers.
10. Secondary Spontaneous:
Secondary spontaneous pneumothorax (SSP) occurs
in people with a wide variety of parenchymal lung
diseases.These individuals have underlying
pulmonary pathology that alters normal lung
structure.
Air enters the pleural space via distended, damaged,
or compromised alveoli. The presentation of these
patients may include more serious clinical symptoms
and sequelae due to co morbid conditions.
chronic obstructive pulmonary disease (COPD)
cystic fibrosis
severe asthma
lung infections, such as tuberculosis and certain
forms of pneumonia
11. sarcoidosis
thoracic endometriosis
Pulmonary fibrosis.
lung cancer and sarcomas
involving the lungs.
12. 2. TRAUMATIC PNEUMOTHORAX
A Traumatic pneumothorax occurs when air escapes
from laceration in the lung field and enters the
pleural space or from a wound in the chest wall. It
may result from :
Blunt trauma (Ribs fracture)
Penetrating chest or abdominal trauma (Stab wounds
or gunshot wounds)
Diaphragmatic tears.
Invasive thoracic procedure: Thoracentesis,
transbronchial lung biopsy, insertion of a subclavian
line.
Barotrauma with mechanical ventilation.
13.
14. A traumatic pneumothorax resulting from major
injury to the chest is often accompanied by
hemothorax. Often both blood and air found in
pleural cavity hemopneumothorax after major
trauma. Chest surgery can be classified as a
traumatic pneumothorax as a result of the entry
into the pleural space and the accumulation of air
and fluid in the pleural space.
15. OPEN PNEUMOTHORAX is one form of
traumatic pneumothorax. It occurs when a wound in
the chest wall is large enough to allow air to pass
freely in and out of the thoracic cavity with each
attempted respiration. Because of the rush of air
through the wound in the chest wall produces a
sucking sound, in such injuries are termed sucking
chest wounds.
In such patient not only does the lung collapse, but
the structures of the mediastenum also shift toward
the uninjured side with each inspiration and in the
opposite direction with expiration. This is the terms
as the medistinal flutter or swing, and it produces
serious circulation problems.
16.
17. 3. TENSION PNEUMOTHORAX
A tension pneumothorax occurs when air is drawn
into the pleural space from a lacerated lung or through
a small opening or wound in the chest walls. It may
be a complication of other types of pneumothorax.
In contrast to open pneumothorax, the air that enters
the chest cavity with each inspiration is trapped; it can
not be expelled during expiration through the air
passages or the opening in the chest wall.
18. In effect, a one way valve or ball valve mechanism
occurs where air enters the pleural space but cannot
escape. With each breath tension (positive pressure) is
increased within the affected pleural space. This causes
the lung to collapse and the heart and great vessels, and
the trachea to shift towards the unaffected side of the
chest known as mediastinal shift.
Both respiratory and circulatory function are
compromised because of the increased intrathoracic
pressure, which decreases venous return to the heart,
causing decreased cardiac output and impairment of
peripheral circulation. In extreme cases, the pulse may
be undetectable this is known as pulse less electrical
activity.
22. CLINICAL MANIFESTATION
Moderate Pneumothorax includes:
Tachypnea
Dyspnoea
Sudden sharp pain on the affected side.
Coughing
Diminished or absent breath sound on the affected
side.
Restless
Anxiety
Tachycardia.
23. CLINICAL MANIFESTATION
Sever Pneumothorax includes:
All the preceding and distended neck veins
Subcutaneous emphysema
Decreased tactile and vocal fremitus;
Tracheal deviation towards the unaffected side
Progressive cynosis.
24.
25. DIAGNOSTIC EVALUATION
Chest radiography: Anteroposterior and/or
lateral decubitus films
Contrast-enhanced esophagography: If
emesis/retching is the precipitating event
Chest computed tomography scanning: Most
reliable imaging study for diagnosis of
pneumothorax but not recommended for routine
use in pneumothorax
Chest ultrasonography
26.
27. MANAGEMENT
Immediate needle decompression for tension
pneumothoraces
Observation and follow-up x-ray for small,
asymptomatic, primary spontaneous
pneumothorax
Catheter aspiration for large or symptomatic
primary spontaneous pneumothorax
Tube thoracostomy for secondary and traumatic
pneumothorax
28. Patients should receive supplemental oxygen until
chest x-ray results are available because oxygen
accelerates pleural reabsorption of air. Treatment
then depends on the type, size, and effects of the
pneumothorax. Primary spontaneous pneumothorax
that is < 20% and that does not cause respiratory or
cardiac symptoms can be safely observed without
treatment if follow-up chest x-rays done at about 6
and 48 h show no progression.
Larger or symptomatic primary spontaneous
pneumothorax should be evacuated by catheter
aspiration. Tube thoracostomy is an alternative.
29. Tube thoracostomy is generally
used to treat secondary and
traumatic pneumothorax.
Symptomatic patients with
iatrogenic pneumothorax are best
managed initially with aspiration.
30. Tension pneumothorax is a medical emergency and
should be diagnosed clinically; time should not be
wasted confirming the diagnosis with a chest x-
ray. It should be treated immediately by inserting a
14- or 16-gauge needle with a catheter through the
chest wall in the 2nd intercostal space at the
midclavicular line.
The sound of high-pressure air escaping confirms
diagnosis. The catheter can be left open to air or
attached to a Heimlich valve. Emergency
decompression must be followed immediately by
tube thoracostomy, after which the catheter is
removed.
31.
32. MEDICATION SUMMARY
A tension pneumothorax requires treatment with rapidity.
However, anesthetics and analgesics should be used if the
patient is not in distress.
The goals of pharmacotherapy are to reduce morbidity and to
prevent complications.
In addition to the medications discussed in this section, talc
may be used as a sclerosing agent for pleurodesis by mixing 2-
5 g in 250 mL of sterile isotonic sodium chloride solution to
form a slurry or poudrage.
Note that acute respiratory distress syndrome (ARDS) has
been reported after use of talc as a pleural sclerosing agent, but
this is considered a rare complication.
33. SURGICAL MANAGEMENT
Thoracotomy
A thoracotomy is a surgical
procedure in which a cut is
made between the ribs to
see and reach the lungs or
other organs in the chest or
thorax. Typically, a
thoracotomy is performed
on the right or left side of
the chest. An incision on the
front of the chest through
the breast bone can also be
used, but is rare. A
thoracotomy is performed
for diagnosis or treatment of
a disease and allows doctors
to visualize, biopsy or
remove tissue as needed.
34. PLEURODESIS
Pleurodesis is a procedure
sometimes performed for
people with pleural effusions
(build-up of fluid between the
membranes surrounding the
lungs) that recur as a result of
lung cancer and other
conditions. In the procedure, a
chemical is placed between the
two membranes that line the
lungs causing them to scar
together. This scarring
obliterates the pleural space so
that fluid can no longer build
up in the space. It is done in the
operating room with a general
anesthetic
36. Complications of surgical procedures include
the following:
Failure to cure the problem
Acute respiratory distress or failure
Infection of the pleural space
Cutaneous or systemic infection
Persistent air leak
Reexpansion pulmonary edema
Pain at the site of chest tube insertion
Prolonged tube drainage and hospital stay
37. NURSING MANAGEMENT
Monitor respiratory status for increase in rate,
decrease in depth, dyspnea, or cyanosis.
Auscultate breath sounds.
Observe for symmetrical chest expansion.
Observe for position of trachea.
Listen for sucking sounds with inspiration; if
present, apply occlusive dressing over wound while
patient performs Valsalva maneuver.
Observe for paradoxical movements of the chest
during respiration; if present, stabilize the flail area
with a sandbag or pressure dressing, and turn to the
affected side.
38. Place patient in semi-sitting position.
Prepare patient for and assist with insertion of chest
tube.
Once chest tube is inserted, ensure that connections
are tightened and taped securely per hospital
protocol.
Monitor water-seal drainage bottles to ensure fluid
level is above drain tube.
Maintain prescribed level of suction to drainage
system.
39. Observe the water-seal drainage system for bubbling.
Monitor drainage system for continuous bubbling and
ascertain if the problem is patient or system-centered.
Clamp chest tube near the patient's chest.
If patient has insertion site air leak, apply vaseline-
impregnated gauze around site, and reassess the
problem.
If patient has drainage system air leak, ascertain the
location by clamping the tube downward toward the
system by increments. Secure connections.
40. Observe for fluid tidaling.
Monitor fluid drainage for character and amount,
and notify MD if drainage is greater than 100 cc/hr
for more than 2 hours.
Strip chest tubes gently, if at all, per hospital
protocol.
Place chest drainage system below the level of the
chest, and coil tubing carefully to avoid kinking
41. Obtain chest x-rays daily.
If chest tube is accidentally removed, apply
vaseline-impregnated gauze and pressure dressing,
and notify MD.
If chest tube becomes accidentally disconnected
from tubing, reconnect as cleanly and quickly as
possible.
Observe dressing over chest tube insertion site for
drainage and notify MD for significant drainage.
42. Assure that chest tube clamps (2 for each tube) are
present in patient's room and are taken with patient
when transported out of unit.
Assist with removal of chest tube as warranted, and
apply vaseline-impregnated gauze and dry sterile
dressing over site, and change per hospital protocol.
Monitor patient for changes in respiratory status,
oxygenation, chest pain, dyspnea, or presence of
subcutaneous emphysema