Everything You Need to Know About Hernias
•Download as PPTX, PDF•
40 likes•16,918 views

Simple notes on definition of abdominal hernias in general, as well as clinical features and management of inguinal hernias. Brief explanation of hernia repair methods (laparoscopic, open surgery)

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Everything You Need to Know About Hernias
Similar to Everything You Need to Know About Hernias (20)
Recently uploaded
Recently uploaded (20)
Everything You Need to Know About Hernias
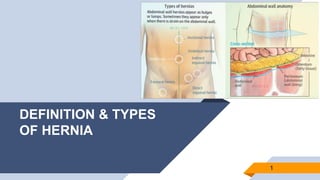
- 1. DEFINITION & TYPES OF HERNIA 1
- 2. “‘HERNIA’ Greek - an offshoot / bulge Latin - to tear / rupture An abnormal protrusion of an organ or part of an organ through a defect / weakness in the wall of the cavity normally containing it 2
- 3. Structural weakness Anatomy, congenital, collagen diseases, aging, neurological & muscular diseases Intra-abdominal pressure Pregnancy, COPD, ascites, tumours,etc. Injury Trauma (Sharp / blunt), surgical incision (defective healing, poor technique) 3 CAUSES
- 4. DEFINITIONS Reducible Contents can be returned to the abdomen when given pressure on. Irreducible Contents cannot be reduced or pushed back into the abdomen but no complication. Mild / absent symptoms Obstructed The herniated part of bowel is irreducible but has good blood supply. 4 Incarcerated Irreducible hernia with viable contents, used synonymously with obstructed hernia. Contents of the hernial sac are stuck to one another by adhesions Strangulated Visceral contents of hernia become twisted or entrapped by narrow opening Compromised blood supply, ischaemic / necrotic contents Painful / tender on palpation Sliding Part of a viscus (e.g. colon) is adherent to the outside of the peritoneum (extraperitoneal) forming the hernial sac beyond the hernial orifice) Usually on the left.
- 5. COMPOSITION OF A HERNIA Sac Mostly the diverticulum of peritoneum (Mouth, neck, body, fundus) Covering of the sac Composed of the layers of abdominal wall through which the sac passes. Contents of the sac Depending on the part of abdomen that is herniated Omentum, intestines, etc. 5
- 6. TYPES OF HERNIA - ANATOMICALLY Based on location ▰Inguinal Hernia ▰Femoral Hernia ▰Umbilical Hernia (14%) ▰Epigastric Hernia (7%) ▰Para-umbilical Hernia ▰Incisional Hernia (9%) ▰Hiatal Hernia ▰Spigelian Hernia 6 }(70%)
- 9. INGUINAL HERNIAS¾ of all abdominal wall hernias 9 Direct Indirect
- 10. DIRECT vs INDIRECT INGUINAL HERNIA 10
- 11. TYPES OF INDIRECT INGUINAL HERNIAS 3) Bubonocele: Hernia does not come out of the superficial inguinal ring and is limited to the inguinal canal. 11 1) Complete Hernia: Hernial sac is patent up to the bottom of the scrotum (males) or labia majora (females). 2) Incomplete Hernia: The process vaginalis sac is patent up to root of scrotum but it comes out through the superficial inguinal ring.
- 12. PHYSICAL EXAMINATION Inspection: ▰Swelling: Pyriform shape extending down – indirect; circular shape – direct; spherical shape, starts from below the inguinal ligament – femoral. ▰Skin: Normal (uncomplicated); erythema (strangulated) ▰Impulses on coughing: Momentary bulge (absent if neck of the sac is obstructed ) Palpation: ▰Non-tender unless strangulated ▰Granular (omentocele); elastic (enterocele) Zieman’s Technique: ▰Differentiate direct/indirect/femoral Method: Place the index finger (indirect) over the deep inguinal ring the middle finger (direct) on the superficial inguinal ring and the ring finger (femoral) over the saphenous opening and ask the patient to Ring occlusion test: ▰Differentiate indirect/direct Method: Performed in standing position, ask patient to cough when thumb is pressed on the deep inguinal ring - bulge medial to thumb (direct) Percussion: ▰Resonance (enterocele); dullness (omentocele or fatty tissue) Auscultation: Not applicable 12 Position of patient: First standing, then lie supine
- 13. CLINICAL FEATURES 13 May be asymptomatic and found incidentally. Site: Groin area Onset: Gradual / acute (incarceration) Character: Burning, gurgling, or aching pain with heavy or dragging sensation in the groin Radiation: Localized, may radiate to the scrotum Associated symptoms: Weakness in groin, (if strangulated) nausea & vomiting, fever and inability to pass gas / stool
- 14. CLINICAL FEATURES (continued) 14 Time / Duration: Constant, worse toward the end of the day or after prolonged activity Exacerbating factors: Worsen with Valsalva maneuvers. Activities that increase intra-abdominal pressure, i.e. coughing, lifting, or straining, cause more abdominal contents to be pushed through the hernia defect. Severity: Mild to severe Progression: Bulge of the hernia gradually increases in size, suddenly intensified pain may indicate strangulation * If bulge disappears while patient is in the supine position, clinical suspicion of a hernia should be increased.
- 15. Hernia repair techniques – indicated in irreducible, symptomatic cases 1) Open or conventional hernia repair 2) Laparoscopic hernia repair Gold standard - Mesh Repair ▰ Hernioplasty – Herniotomy plus reinforcement of the posterior wall of the inguinal canal with a synthetic mesh ▰ Herniorrhaphy – Herniotomy plus repair of the posterior wall of the inguinal canal ▰ Herniotomy – Removal of hernia sac without any repair of the inguinal canal MANAGEMENT OF INGUINAL HERNIA 15
- 16. OPEN INGUINAL HERNIA REPAIR Mesh inserted to cover and support the posterior inguinal canal. (Hernioplasty) 16 * PHS – PROLENE hernia system Before After
- 17. 17 LAPAROSCOPIC INGUINAL HERNIA REPAIR Performed under GA, extra-/ trans-peritoneally. Not appropriate for large or irreducuble hernias.
- 18. ADVANTAGES OF REPAIR TECHNIQUES ▰Laparoscopic repair: ▻ Faster recovery times ▻ Less risk of long-term pain ▻ Lower risk of another hernia recurrence after a previous recurrence ▰Open hernia repair: ▻ Fewer internal injuries ▻ Lower recurrence rates in the context of primary inguinal hernia 18
Editor's Notes
- if the sac is direct the neck is going to be wide, but in case of indirect inguinal hernia the neck is going to be narrow and there is increase chance of strangulation which can lead to ischemia and necrosis, in case of direct and incisional hernia no neck is present. sometime there is no sac present like in case of Epigastric hernia.