Here are the key points for Case Scenario 2:- Reasons for short stature: - Growth hormone deficiency - Constitutional delay of growth - Familial short stature- Best test to diagnose GH deficiency: IGF-1 levels- Three further investigations: - Insulin tolerance test - GHRH + arginine stimulation test - MRI pituitary to rule out structural abnormalitiesThe diagnosis is Growth Hormone Deficiency based on the clinical features of short stature, thin skin, decreased muscle mass and social/behavioral issues. IGF-1 levels would help to confirm the diagnosis. Dynamic stimulation tests can further establish the growth hormone deficiency. MRI pituitary is recommended to
•Download as PPSX, PDF•
16 likes•10,240 views

by West Medical Ward King Edward Medical University , Lahore, Pakistan.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (13)
Similar to Here are the key points for Case Scenario 2:- Reasons for short stature: - Growth hormone deficiency - Constitutional delay of growth - Familial short stature- Best test to diagnose GH deficiency: IGF-1 levels- Three further investigations: - Insulin tolerance test - GHRH + arginine stimulation test - MRI pituitary to rule out structural abnormalitiesThe diagnosis is Growth Hormone Deficiency based on the clinical features of short stature, thin skin, decreased muscle mass and social/behavioral issues. IGF-1 levels would help to confirm the diagnosis. Dynamic stimulation tests can further establish the growth hormone deficiency. MRI pituitary is recommended to
Similar to Here are the key points for Case Scenario 2:- Reasons for short stature: - Growth hormone deficiency - Constitutional delay of growth - Familial short stature- Best test to diagnose GH deficiency: IGF-1 levels- Three further investigations: - Insulin tolerance test - GHRH + arginine stimulation test - MRI pituitary to rule out structural abnormalitiesThe diagnosis is Growth Hormone Deficiency based on the clinical features of short stature, thin skin, decreased muscle mass and social/behavioral issues. IGF-1 levels would help to confirm the diagnosis. Dynamic stimulation tests can further establish the growth hormone deficiency. MRI pituitary is recommended to (20)
More from KemUnited
More from KemUnited (20)
Recently uploaded
Recently uploaded (20)
Here are the key points for Case Scenario 2:- Reasons for short stature: - Growth hormone deficiency - Constitutional delay of growth - Familial short stature- Best test to diagnose GH deficiency: IGF-1 levels- Three further investigations: - Insulin tolerance test - GHRH + arginine stimulation test - MRI pituitary to rule out structural abnormalitiesThe diagnosis is Growth Hormone Deficiency based on the clinical features of short stature, thin skin, decreased muscle mass and social/behavioral issues. IGF-1 levels would help to confirm the diagnosis. Dynamic stimulation tests can further establish the growth hormone deficiency. MRI pituitary is recommended to
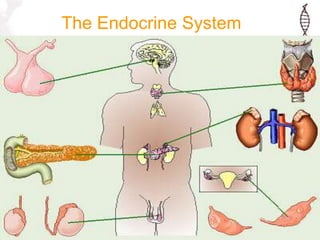
- 2. Endocrine Disorders • Disease states that result from excess or insufficiency of hormone • Clinical challenge is determination of the origin of excess or insufficiency, i.e., Hypothalamus (tertiary), Pituitary (secondary) or target gland (primary)
- 3. Endocrine Disorders (Other than diabetes) • Thyroid • Adrenal • Parathyroid • Pituitary gland • Gonadal • Gout (uric acid)
- 4. Hypothalamus ACTH = adrenocorticotropic hormone LH = lutenizing hormone FSH = follicle-stimulating hormone AVP = arginine vasopressin CRH = corticotropin-releasing hormone GHRH = growth hormone-releasing hormone GnRH = gonadotropin-releasing hormone GH = growth hormone TSH = thyroid-stimulating hormone PRL = prolactin SRIF = somatotropin release–inhibiting factor (somatostatin) TRH = thyrotropin-releasing hormone; VIP = vasoactive intestinal polypeptide. DA = dopamine Goldman: Cecil Medicine, 23rd ed. 2007
- 5. Hormone Target Gland Growth hormone (GH) Multiple Prolactin (PRL) Breast Adrenocorticotropic hormone (ACTH) Adrenal Thyroid-stimulating hormone (TSH) Thyroid Luteinizing hormone (LH) Gonad Follicle-stimulating hormone (FSH) Gonad Anterior Pituitary Hormones
- 6. Anterior Pituitary Hormones • TSH, ACTH, FSH, and LH hormones are tropic hormones that simulate other endocrine glands • TSH-Thyroid • ACTH- Adrenal Cortex • FSH, LH- Gonads
- 7. Posterior Pituitary Hormones • Vasopressin(ADH)- kidney, baroreceptors (plasma osmolality, water retention, thirst) • Oxytocin- breast, uterus (no known function in males) • Both are synthesized in specialized neurons in the hypothalamus (neurohypophyseal neurons)
- 8. Too big, Too tall or Too short Prof. Tariq Waseem
- 10. CASE SCENARIO 1 • A 50 yr old male presented in OPD with C/O off & on headache, poor concentration and fatigue. He has gained weight, he sweats a lot. He also has difficulty in churning the food bolus in mouth and food particles are stuck in his unusually widened teeth spaces. His skin has coarsened and has developed multiple skin tags. His friends report that he has a heavy, doughy and sweaty handshake and often does not notice people sitting on either sides of his desk.
- 11. • O/E • BP 160/100. • Displaced cardiac apex in 6th i.c. space. • Hepatosplenomegaly. • BSR 240mg/dl • Glycosuria ++
- 13. • What is the diagnosis? • What is the best test to diagnose this condition? • List three further investigations to confirm the diagnosis.
- 14. GROWTH HORMONE •Single chain 191 amino acid anabolic polypeptide synthesized by somatotropic cells of anterior pituitary gland. •Fasting serum values <5ng/ml
- 15. BIOREGULATION & EFFECTS GHRH, Ghrelin Sex hormones Sleep, fasting, exercise, arginine Somatostatin Hyperglycemia Glucocorticoid IGF RAISED IGF – Impair insulin sensitivity. HYPERGLYCEMIA- breakdown of pancreatic islets
- 16. CAUSES OF GH-DEFICIENCY GH-EXCESS • CONGENITAL ABNORMALITIES • INTRACRANIAL TUMORS (CRANIOPHRANGIOMA) • IRRADIATION, SURGERY OR TRAUMA • SHEEHAN SYNDROME • AUTOIMMUNE •MICRO OR MACROADENOMAS •IN ASSOCIATION WITH MEN-I •RARELY BY ECTOPIC GHRH
- 17. ACROMEGALY ACROMEGALY is a condition in adults caused by hyper secretion of GH hormone after the closure of epiphyseal plates. GIGANTISM occurs if growth hormone excess starts in in children or adolescents before epiphyseal closure. GIGANTISM
- 18. Epidemiology • Acromegaly is more common than gigantism, with an incidence of 3-4 cases per million people per year and a prevalence of 40-70 cases per million population.
- 19. Genetics • In gigantism inherited and manifested during childhood or adolescence GPR101, a gene on the X chromosome, is overexpressed. • A mutation in the GPR101 gene was found in about 4% of cases of Acromegaly. • The GPR101 gene may be a target for the treatment of growth disorders.
- 20. SIGNS & SYMPTOMS
- 21. SIGNS & SYMPTOMS
- 23. COMPLICATIONS Hypopituitirsm Visual defects Hypertension Glucose intolerance/ frank DM Cardiomegaly / cardiac failure Carpal tunnel syndrome Cord compression Colon polyps
- 24. LABS Serum Growth Hormone (Unreliable) Raised IGF-I, IGF binding protein IGFBP-3 Hypercalcemia Hyperphosphatemia T4 & TSH Low (secondary hypothyroidism) Hyperprolactinemia(mammosomatotrophs are the most common type of GH-secreting cells involved in childhood gigantism Hyperglycemia GLUCOSE TOLERANCE TEST A 75g glucose syrup is given orally and serum GH levels are measured @ 60, 90, 120 min. ACROMEGALY is excluded when levels are < 1ng/ml
- 26. IMAGING X-Ray Hands X-Ray Skull Lat. MRI Pituitary
- 28. TREATMENT • 1ST Line PITUITARY MICROSURGERY • 2ND Line RADIOSURGERY • 2nd Line MEDICAL Somatostatin analogue Dopamine agonist GH receptor antagonists
- 29. MICROSURGERY • Trans sphenoidal hypophysectomy has the dual advantage of rapidly improving symptoms caused by mass effect of the tumor and significantly reducing or normalizing GH/IGF-I concentrations.
- 30. RADIOTHERAPY • External radiotherapy is given in cases of remissions after surgery. • Gamma Knife Surgery • Associated with risks of panhypopitutirsm.
- 31. MEDICAL THERAPIES As 2nd line therapy after surgery to reduce GH levels < 5mU/l DOPAMINE AGONISTS CABERGOLINE effective in tumors secreting both prolactin & GH. SOMATOSTATIN ANALOGUE OCREOTIDE & lanreotide given as s/c injections. GH RECEPTOR ANTAGONISTS PEGVISOMANT is used primarily for symptomatic relief.
- 32. Treatment • Cure, or adequate control, of growth hormone (GH) excess is defined as a glucose-suppressed GH concentration of less than 2 ng/mL, as determined by radioimmunoassay (1 mcg/L by IRMA), and normalization of the serum insulinlike growth factor I (IGF-I) concentration.
- 33. Summary Acromegaly is a rare, insidious, and potentially life-threatening condition for which there is good, albeit incomplete, treatment that can add years of high-quality life for the patient. Increased and unregulated growth hormone (GH) production, usually caused by a GH- secreting pituitary tumor (somatotroph tumor), characterizes acromegaly.
- 35. • What is the diagnosis? • What is the best test to diagnose this condition? • List three further investigations to confirm the diagnosis.
- 36. Stockholm Sweden
- 37. CASE SCENARIO 2 • A mother brings her 15 yr old son to the OPD complaining he has not gained height compared with his siblings and classmates. He is depressed and feels socially isolated. He is 3.5 ft tall with thin skin and wrinkles, decreased body tone. His mother complains of his unsocial behavior at home and lack of interest in studies. • What can be reasons of his short stature?
- 38. DIFFERENTIALS • Familial short stature • Constitutional delay • GH deficiency • Achondroplasia • Vitamin D deficiency • Sex hormone deficiency
- 39. PROPOTIONATE DIS PROPPORTIONATE TYPES OF DWARFISM
- 40. SIGNS & SYMPTOMS OF GH- DEFICIENCY •Retarded growth •Central obesity •Psychogenic symptoms •Decreased bone and muscle mass •Thin skin with fine wrinkles •Poor sweating or temperature regulation •Decreased energy and endurance •Low energy levels •Increased cholesterol and LDL •Increased systolic blood pressure •Decreased cardiac output •Overproduction of insulin
- 41. Lab tests for GH Deficiency • LOW IGF-I LEVELS • INSULIN TOLERANCE TEST • GHRH + ARGININE STIMULATION TEST AVOID IN PTS WITH SEIZURES & CAD AVOID IN PTS WITH KIDNEY &LIVER DISEASE
- 42. LARON SYNDROME • Autosomal recessive disorder due to mutations in the gene for GH receptor. • Resistance to GH resulting in IGF-I DEFICIENCY. • Show resistance to DIABETES. •Dwarfism •Depressed nasal bridge •Underdeveloped mandible •Central obesity •Hypoglycemic seizures BIOSYNTHETIC IGF-I BEFORE PUBERTY