
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Managment of labor for undergraduate
Similar to Managment of labor for undergraduate (20)
More from Faculty of Medicine,Zagazig University,EGYPT
More from Faculty of Medicine,Zagazig University,EGYPT (12)
Recently uploaded
Recently uploaded (20)
Managment of labor for undergraduate
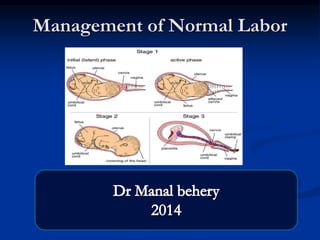
- 1. Management of Normal Labor
- 3. Full history: 1-Complete obstetric history. 2-History of the present pregnancy. 3-History of the present labor ( e.g.: labor pains, vaginal bleeding, gush of fluid& fetal movement).
- 4. General Examination: Vital signs ( pulse , B.P. , temperature,…etc.)
- 6. Fundal level
- 7. Fundal grip
- 11. Palpation
- 12. Auscultation
- 13. 3-Pelvic examination: Cervix : dilatation (c.m.), effeacemet (%) , position & consistency. membrane: intact or ruptured ( if ruptured exclude cord prolapse). -Amniotic fluid ( after R.O.M.): either clear , meconium stained or blood stained. -Presenting part , position ,station & moulding. -Assessment of pelvic capacity
- 14. Cervical dilatation It is the surest way to assess progress of labour
- 15. Assessment of pelvic capacity
- 19. Partograph a graphical record of the observations made of a women in labor For progress of labor and conditions of the mother and the fetus
- 20. History Of Partogram Friedman's partogram
- 21. latent phase Starts from onset of labour until the cervix reaches 3 cm dilatation lasts 8 hours or less Contractions at least 2/10 min contractions each lasting < 20 seconds
- 22. Active phase : The cervix should dilate at a rate of 1 cm / hour or faster Contractions at least 3 / 10 min each lasting < 40 seconds
- 23. Closed cervix vs effeced vs dilated Cx
- 24. Components of the partograph Part 1 : fetal condition ( at top ) Part 2 : progress of labour ( at middle ) Part 3 : maternal condition ( at bottom )
- 25. Part 1 : Fetal condition Recording fetal heart rate
- 26. Membranes and liquor Dilated cervix with bag of fore water I: intact C : clear M : muconium B : blood stained
- 27. Molding the fetal skull bones . Increasing molding with the head high in the pelvis is an ominous sign of Cephalopelvic disproportion. separated bones . sutures felt easily……….O bones just touching each other……………..+ overlapping bones …………… …………...++ severely overlapping bones ( notable ) ……..+++
- 28. Part 2 – progress of labour . Cervical dilatation: it is divided into a latent phase and an active phase Descent of the fetal head Uterine contractions
- 29. Descent of the fetal head The rule of fifth BY abdominal examination
- 30. Assessing descent of the fetal PV; 0 station is at the level of the ischial spine
- 32. Engagment
- 33. Normal progress in labor
- 34. Alert line ( health facility line ) The alert line drawn from 3 cm dilatation represents the rate of dilatation of 1 cm / hour Moving to the right or the alert line means referral to hospital for extra care
- 35. Action line ( hospital line ) The action line is drawn 4 hour to the right of the alert line and parallel to it This is the critical line at which specific management decisions must be made at the hospital
- 36. When labor goes from latent to active phase , plotting of the dilatation is immediately transferred from the latent phase area to the alert line
- 37. Normal labor progress At addmision Then after 4h
- 40. PART 3:Recording of maternal condition
- 41. -
- 42. Management of the first stage
- 43. Ambulating and position in labor Walking may be more comfortable than being supine during early labor The left lateral position keeps the uterus off the inferior vena cava; this prevent (supine hypotensive syndrome)
- 46. Evaluation of fetal well-being Measurement of the fetal heart rate By hand-held Doppler, or By CTG
- 47. Late in first stage patients may report the urge to push. This may indicate significant descent of the fetal head with pressure on the perineum.
- 48. Management of the second stage
- 49. Diagnosis of the onset of the 2nd stage Feeling a desire to evacuate the bladder or rectum Reflex desire to bear down during contractions. The uterine contractions are more prolonged and vigorous. Full cervical dilatation (the surest sign).
- 50. Transport the lady to the delivery room. . (A)Position: - Lithotomy position or Dorsal position. (B)Paint vulva & perineum with antiseptic solution. (C)Apply sterile leggings and towels (D)Evacuate the bladder by catheter (if not evacuated before)
- 51. Litotomy positionVS dorsal position
- 52. F)Ask the lady to bear down during uterine contractions and relax in between. J). V oxytocin drip in glucose solution 5% may be given.
- 53. 4)The main task of the obstetrician is to prevent perineal lacerations, how?
- 54. When the labia start to be separated by the head, put a sterile dressing on the perineum and press on it during uterine Contractions.
- 55. A. Support of the perineum till crowning occurs
- 56. Crowning: The B.P.D passes through the vulval ring during contraction and the head does not recede inbetween uterine contractions.
- 57. Episiotomy when the perineum is maximally stretched and about to tear
- 58. Problems arising from Episiotomy 58 Pain Edema Bleeding Infection Defects in wound
- 60. B. After crowning, Prevent straining after crowning. Allow gradual and slow extension only inbetween uterine contractions. by doing "Rtigen maneuver“
- 61. Examine neck for looped umbilical cord . If a loop of cord is coiled around the neck Try to slip it. If several loops, apply double clamping and cut the cord inbetween.
- 62. Support infant’s head as it rotates for shoulder presentation . Guide infant’s head downward to deliver anterior shoulder
- 63. 7)Deliver posterior shoulder first , then the anterior shoulder when the anterior shoulder appears under the pubic arch,the head is lifted upwards to deliver the posterior shoulder, then downwards to deliver the anterior shoulder.
- 64. The rest of the body usually slips easily
- 65. 8)Hold the fetus from its feet Contraindications 1-Premature baby 2-Fetal asphyxia 3-Suspected presence of intracranial hemorrhage.
- 66. 9)Milking the cord Towards the fetal umbilicus add l00 cc of blood to fetal circulation Alternatively, the infant is held about half minute below the level of the vaginal introitus before clamping the cord.
- 67. In cases of Rh incompatibility The cord should be clamped immediately with no milking to avoid addition of more bilirubin from destructed R.B.Cs to fetal circulation →more hyperbilirubinaemia
- 68. 10)Clamp the cord by 2 ring forceps and cut inbetween After delivery and evaluation of infant, clamp and cut cord
- 69. D- Management of the 3rd Stage: Normally the placenta is expelled within 10 minutes, if expelled between 10- 30 minutes (delayed delivery of placenta). If not expelled within 30 minutes (Retained placenta).
- 70. Active management of 3rd stage of labor. A CONTROLLED CORD TRACTION
- 74. Physiological Management Passive or expectant management No prophylactic oxytocics Cord clamped after delivery of placenta No Controlled Cord Traction (CCT)
- 76. check placenta and membranes for completeness and normality
- 77. THANK YOU
- 79. The aim of active management of labour is to ensure that the primigravida will deliver a healthy baby in less than 12 hours
- 80. Benefits of Active Management of Labour It avoids prolonged labour which can lead to: Maternal distress and emotional upset. Fetal hypoxia and distress. Exhaustion of the medical and nursing staff.
- 81. The Principles of Active Management of Labour
- 82. 1-Antenatal education :The mother is informed about the physiology of labour and assured that labour will take less than 12 hours. In this way, she can cope better with the stress of labour.
- 83. 2-Strict diagnosis of onset of labour. Onset of regular involuntary coordinated, painful uterine contractions associated with cervical effacement and dilatation
- 84. 3-Regular follow-Up of the Patient during Labour : PV is done on admission to the labor. This will be repeated every 1-2 hours
- 86. 4-Correction of Abnormal Progress The rate of cervical dilatation should not be less than 1 cm per hour in the active phase of labour. If the cervix is not dilating properly, amniotomy or pitocin drip
- 88. 5-Personal Attention: one nurse face to face for each patient .
- 89. 6-Diet Nothing is allowed by mouth.
- 90. 7-Provision of suitable analgesia.