2. Introduction
• Ataxia = from Greek- a- [lack of]+ taxia [order]
• Rate, rhythm and force of contraction of voluntary movements
• Disorganized, poorly coordinated, or clumsy movements
Traditionally used specifically for lesions involving
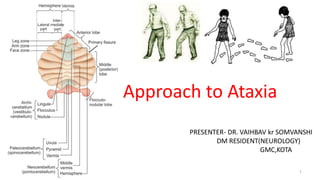
• Cerebellum or it’s pathways
• Proprioceptive sensory pathways
7. Sensory Ataxia
• Loss of distal joint, position sense
• Absence of cerebellar signs such as dysarthria or nystagmus
• Loss of tendon reflexes
• Corrective effects of vision on sensory ataxia
• Romberg sign
8. Vestibular Dysfunction
• Vertigo is prominent
• Consistent fall to one side
• Nystagmus
• Limb ataxia is absent
• Speech is normal
• Joint position sense is normal
9. Approach to ataxic patient
Meticulous evaluation of History
Age at Onset
Course of disease
Drug intake
Family History
Personal Social & Occupational information
Distribution of ataxia
History of other system illness
Neurological evaluation
Ancillary tests
9
11. • Drug intake
– Phenytoin, barbiturates, lithium, immunosuppressants (methotrexate,
cyclosporine), chemotherapy (fluorouracil, cytarabine)
• Family history
– Study at least 3 generations
– Consanguinity
– Ethnicity
• Social/Occupational History
– Alcohol and drug use, toxins (heavy metals, solvents, thallium), smoking
(Vascular)
History
11
12. Distribution of ataxia
• Symmetric - Acquired, Hereditary, degenerative ataxias
• Asymmetric- Vascular, Tumors, demyelinating, Infection, congenital causes
Other system illness
• Gastrointestinal symptoms- gluten ataxia
• Mass lesion- paraneoplastic ataxias
History
12
13. Children
• Refusal to walk or with a wide-based, "drunken" gait.
• Vertigo, dizziness and vomiting
• Personality and behavioral changes.
• Abnormal mental status
• A history of head trauma ,neck trauma
• Patients with a recent infection or vaccination
• Previous similar episodes of acute ataxia.
• Children with family members with ataxia
13
14. Examination
Neurological examination
• Ataxia (appendicular or axial)
• Dysmetria
• Dysdiadochokinesia
• Rebound Phenomenon
• Dysarthria
• Tremor
• Titubation and increased postural sway
• Hypotonia
• Nystagmus
• Other system evaluation
Breast Lump, mass per-abdomen etc.
14
36. 36
Cerebral Sensory frontal
Base of support Wide base Looks down Wide base
Velocity Variable Slow Very slow
Initiation Normal Normal Hesitant
Turns Unsteady Unstaedy Hesitant,multiple steps
Postural instability + + +++++
Falls Late event More in night Frequent
Heel shin Abnormal Abnormal,difficulty in
point of initiation
Normal
Types of Ataxia
37.
38. Management
• Corrective measures for deficiencies – Vitamin E, Thiamine
• Specific diet – Gluten free diet, ketogenic diet
• Immunologic disorder – IVIG, Plasmapharesis
• Miglustat for niemann pick disease
• Riluzole – hereditary and degenerative ataxia and dysarthria
• Varenicline – SCA3
• 4- aminopyridine, Acetazolamide – Episodic ataxia type 2
• Nicotinamide, deferiprone, idebenon – friedreich ataxia, mitochondrial ataxia
• Rehabilitation, exercise help in SCA type 1
• Zinc supplementation and DBS also help in SCA 2
• Actimmune – IFN-γ analogue morbidity benefit for friedreich ataxia
• Antisense oigonuceotide shown to knock down toxic protein level in SCA 2 and 3 mouse model
38
39. Case Scenario
55-year-old man presented with progressive gait difficulty. He had initially noted difficulty
walking downstairs, upstairs and running at the age of 47. His imbalance problems became
progressively worse over the years, and he developed slurred speech, transient double vision
while turning his head quickly, and loss of hand dexterity. He had frequent falls and needed to
use a walker. He had an extensive family history of cerebellar ataxia, affecting his mother and
brother. On examination, he had slurred speech and slow saccadic eye movements without
nystagmus or hypermetric or hypometric saccades. He had dysmetria on finger-nose-finger
tests and overshoot in finger chase tests. He also had impaired rapid alternating movements
with absent reflexes in upper limb and hyporelexia in lower limb. He had a hypomimic facial
expression and bradykinesia left side with retropusion test positive. His gait showed variable
stride length and was wide based.
39
41. Genetic tests - 38 repeats CAG expansions of the ATXN2 gene (normal <32),
Diagnosed as SCA 2
The patient treated with riluzole 50 mg 2 times a day which
provided modest benefits for his speech. Physical therapy helped with
his balance. Carbidopa/levodopa 25 mg/100 mg, 3 times a day, improved
his parkinsonism by increasing the speed of her movements.
41
42. Conclusion
An approach to ataxia is based on knowledge of its symptoms and
causes
Knowledge of differentiating clinical features takes clinicians closer to
the etiological diagnosis which help in investigational decisions.
Treatable causes must be identified and ruled out
Genetic testing is prudent for providing better insight into the
management.
• On going clinical trials for management of hereditary and degenerative
ataxias will help in better morbidity outcome of these diseases.
42
43.
44. • Bradley’s Neurology in clinical Practice,eighth edition
• Handbook of Clinical Neurology, Vol. 103 (3rd series), Ataxic Disorders
• http://www.ataxia.org -National Ataxia Foundation web site
• http://www.ncbi.nlm.nih.gov/books/NBK1138/ Detailed information about ataxias
• http://www.clinicaltrials.gov –clinical trials information
• Pubmed-with the searchterms “spinocerebellar ataxia”,“Friedreich’s ataxia”, “sporadic ataxia”,“sensory
ataxia”, “approach to ataxia”, “ataxiadiagnosis”
• The Cochrane Library
• Continuum movement disorder 2016
• Continuum movement disorder 2019
• prabhakar_sudesh_singh_gagandeep_eds_differential_diagnosis chapter 22 pg.no.251
References
44
45. Genotype-Phenotype correlations in SCA2
Higher repeats are associated with earlier onset
Homozygous expansion- no increase in severity
Allelic variations of RAI 1 and CACNA1A influences age at onset
Disease duration X CAG length affects occurrence of slow saccades,
Fasciculation, Amyotrophy, Areflexia and Vibration senses
Small disease alleles (32-37): Postural Tremors and Parkinsonism, late onset disease
Medium Size alleles (38-44) : Ataxia, areflexia and slowing of saccades
Large Size Alleles (>45) : Onset <20 years, Chorea and dementia
Higher Size Alleles (>91) : Ataxia, Dystonia, Myoclonus, Cardiac failure, optic atrophy
46. Genotype-Phenotype correlations in
SCA1
Higher repeats are associated with earlier onset and severe disease
Homozygous expansion- no increase in severity
Small disease alleles (39-44) interrupted: Mild Phenotype, Ataxic/non ataxic
features
Medium Size alleles (39-50) Pure CAG: Ataxia and Pyramidal
syndrome
Large Size Alleles (>50) Pure
CAG:
Ataxia and Pyramidal
syndrome &
Amytrophic Lateral sclerosis
Higher Size Alleles
(>91):
Juvenile
disease
47. Genotype-Phenotype correlations in
SCA3
Earlier onset with Higher repeats and inverse
correlation
Homozygous expansion- confers increasing
severity
Small disease alleles (52-73): Axonal Neuropathy and Parkinsonism (Type-III MJD)
Medium Size alleles (73-80) : Ataxia and Diplopia (Type-II MJD)
Large Size Alleles (80-86) : Ataxia, Dystonia and spasticity (Type-I MJD)
Higher Size Alleles (>86) : Rare cases predominant Dystonia (Type-IV)
48. Genotype-Phenotype correlations in
SCA7
Earlier onset with higher repeats and anticipation
Greater expandability during transmission of alleles
Recurrent denovo expansions
Small disease alleles (36-41): Cerebellar ataxia without Retinal involvement
Medium Size alleles (42-49) : Ataxia preceedes Vision diminution Large Size
Alleles (49-60) : Vision loss preceedes Ataxia Higher Size Alleles (>80)
: Juvenile Onset
Extreme High Length Alleles : Infantile Onset, Developmental failure, Multisystem
involvement (>200)
Editor's Notes
Red nucleus
Infeior olivary nucleus
Contralateral detate nuceus
Organ of 3
30 seconds
Peripheral vestibular – fatiguable nystagmus- vertigo better with affected ear up while sleeping
Central vestibular – fast component away from the eccentric side
Symmetrical/ unilateral
SCA 12 north india 1,2,3,7
SCA 6 japanes
Congenital – Arnold chiari malformation
Intention, action
Cerebellar Hypotonia aka gamma spasticity (preserved reflexes) Gamma alpha coordination failure
Occular flutter – to and froth saccading movement like square wave jerk without pause
Opsoclonus – chaotic continuous multidirectional rapid eye movement
Suare wave jerk- opposite direction saccadic eye movement more than 0.3degree with no movement in between ( >10 movement – abnormal)
Ataxia with oculomotor apraxia
Repeat sequencing
WGS
Anti GQ1 ab - MFS
Murcury, bismuth, lead
Low CSF glucose – glucose transporter type 1 deficiency
AFP – AOA 1, 2
AD = autosomal dominant; AR = autosomal recessive; FXTAS = fragile X tremor-ataxia syndrome; GAD =
glutamic acid decarboxylase; ILOCA = idiopathic late-onset cerebellar ataxia; MRI = magnetic resonance
imaging; MSA = multiple system atrophy; REM = rapid eye movement; SCA = spinocerebellar ataxia.
Genetic analyses should be directed according to the frequency of genetic subtypes in the relevant ethnic background (figure 1) and with regard to clinical features.
Axial T2-weighted MRI sequence shows the hot cross bun sign - multiple system atrophy
selective loss of myelinated transverse pontocerebellar fibers and neurons in the pontine raphe with preservation of the pontine tegmentum and corticospinal tracts.
May be seen in SCA 2
SCA 3
Vcjd
HIV related PML
Axial T2-weighted brain MRI demonstrates hyperintensities in the bilateral inferior olivary nuclei - POLG ataxia. SANDO syndrome – POLG mutation - sensory ataxia neuropathy dysarthria ophthalamoplegia
Sagittal T1-weighted brain MRI spinal cord atrophy but no cerebellar atrophy - Friedreich ataxia
(GRE) axial brain MRI show hypointensity surrounding the brainstem, cerebellum, and spinal cord - superficial siderosis.
Fragile X tremor-ataxia syndrome. Axial T2- weighted MRI symmetric increased signal within the MCP.
axial T2-weighted MRI slices demonstrate linear hypointensity in the pons.
autosomal recessive spastic ataxia of Charlevoix-Saguenay showing degeneration of the corticospinal tract
Joubert syndrome. delayed milestones, a prominent forehead and low-set ears,
and cerebellar ataxia, hypotonia, and hyperreflexia, showing dysgenesis of the
isthmus (the part of the brainstem between the pons and inferior colliculus),
thick superior cerebellar peduncles, and hypoplasia of the vermis- molar tooth sign.
Sign also seen – hepatic fibrosis, nephronopthisis, cogan’s syndrome, pontine tegmental cap dysplasia
Anti-Ri
Loss of frataxin function in mitochondria
leads to iron-sulfur cluster deficits, impaired
oxidation, and iron accumulation.
Nicotinamide has been shown to increase
frataxin but no clinical benefit
iron chelator deferiprone and
the antioxidant idebenone are unclear
on long-term benefit with side effect of heart muscle injury.
Idebanon – Co-enzyme Q analogue
Brain MRI showed pontocerebellar atrophy
Axial(SPECT) - SCA 2 shows a marked symmetrical reduction of dopamine transporter binding in the caudate nucleus and putamen.
18-FDG PET - SCA2. Representative sagittal (top), coronal (mid) and axial (bottom) images of 18F-fluorodeoxyglucose uptake show diffusely decreased hypometabolism in the cerebellar cortex and dentate nuclei (mid and bottom images). Note in the SCA2 patients, the decreased tracer uptake in the basis pontis and medulla oblongata as well
![Introduction
• Ataxia = from Greek- a- [lack of]+ taxia [order]
• Rate, rhythm and force of contraction of voluntary movements
• Disorganized, poorly coordinated, or clumsy movements
Traditionally used specifically for lesions involving
• Cerebellum or it’s pathways
• Proprioceptive sensory pathways](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)