Management of Parotitis
•Download as PPTX, PDF•
29 likes•20,854 views

The basics for managing patients with Parotitis linkedin.com/in/robbieschaack

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Management of Parotitis
Similar to Management of Parotitis (20)
Recently uploaded
Recently uploaded (20)
Management of Parotitis
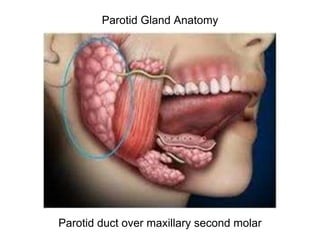
- 1. Parotid Gland Anatomy Parotid duct over maxillary second molar
- 2. nd supply motor innervation to the muscles of facial expression, as well as to the postauricula
- 4. Pathophysiology • decreased salivary production or an impedance of its delivery. • failure of sufficient ductal lavage by saliva facilitates an ascending duct infection from the oral cavity. • infection results in immune/inflammatory response
- 5. Causes • Viral infection from: HIV, Mumps • Bacterial infection from: • medications that cause dry mouth. When your flow of saliva is reduced, bacteria can collect and grow in the Parotid duct. • Dehydration • poor oral hygiene • Sialoliths • Sjögren's syndrome • tumor - can block the flow of saliva (usually not cancerous) • Pneumoparotitis - air gets into the ducts of the parotid gland, most commonly occurs in wind instrument players, glass blowers, and scuba divers.
- 6. Findings • Subjective: • oral or facial pain, especially when eating • abnormal, foul tastes • dry mouth • fever may be present • Objective: • facial asymmetry caused by unilateral parotid gland swelling • Palpation reveals that the swelling is tender and indurated and follows the anatomical contour of the parotid gland. • erythema over skin overlying the glands • Intraorally, a flow of saliva mixed with pus will be seen exiting from the involved parotid duct orifice when the gland is forcefully massaged.
- 7. Diagnosis • Med Hx (medications, Sjögren's, HIV) • Physical exam (pain, swelling, purulence, dry mouth) • Radiographs: PA, Pano, or CT
- 8. nd black arrow indicates a ghost image of the radiopacity on the right side appearing higher and more blurred than its source on the left side. B. Th Imaging Sci Dent. 2013 Sep;43(3):163-169. English. Published online Sep 23, 2013. http://dx.doi.org/10.5624/isd.2013.43.3.163
- 9. Figure 1 Chronic parotitis in the left parotid gland. The computerized tomographic scan demonstrates increased parenchymal density of the left parotid gland (arrow) compared with the right parotid gland. LOUIS MANDEL , ERIN LEIGH WITEK Chronic parotitis : Diagnosis and treatment The Journal of the American Dental Association, Volume 132, Issue 12, 2001, 1707 - 1711 http://dx.doi.org/10.14219/jada.archive.2001.0125
- 10. An oropharyngeal examination reveals dry oral mucosa and swelling adjacent to the right parotid papilla, with no saliva expressed from the orifice (Panel A, arrow). Maxillofacial computed tomography showed changes consistent with inflammation in the parotid gland and surrounding tissues, with marked dilatation of the parotid duct (Panel B, red arrow) and a small calcified mass (Panel B, white arrow) proximal to the duct orifice. Susarla, Peacock, M.D., D.M.D. Obstructive Parotitis. N Engl J Med 2012; 366:2305. June 14, 2012 DOI: 10.1056/NEJMicm1113977
- 11. Treatment • In some cases, no treatment is needed. • Conservative/Palliative treatment: • good oral hygiene (can add Peridex if needed) • stimulate glands by chewing sugarless chewing gum or sour candy (sugarless lemon drops) • massage the gland with heat • increased fluid intake • Antibiotics may be helpful. • Avoid tobacco • Analgesics if needed • In severe cases: superficial parotid lobectomy
- 13. Complications • Prognosis: good! Treatments for most salivary gland infections will go away on their own or are cured with treatment. Complications are not common. • Possible Complications: • Infection recurs • Abscess of salivary gland • spread of infection (cellulitis, Ludwig's angina)
- 14. Conclusion • Dentists are in the unique position to diagnose a patient with Chronic Parotitis. • The ability to perform a thorough clinical examination, salivary examination and imaging procedure facilitates the differentiation of Parotitis from other pathology. • Accurate diagnosis is necessary for an appropriate therapeutic approach.
- 15. Robbie Schaack Doctor of Dental Surgery