Chronic renal failure concise long case approach & crf with fluid overload mx pathway
•
11 likes•2,465 views


Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Chronic renal failure concise long case approach & crf with fluid overload mx pathway
Similar to Chronic renal failure concise long case approach & crf with fluid overload mx pathway (7)
More from Dr. Rubz
More from Dr. Rubz (20)
Chronic renal failure concise long case approach & crf with fluid overload mx pathway
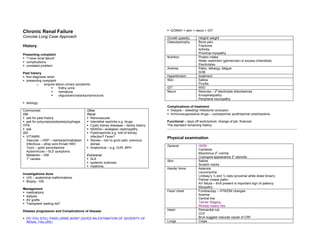
- 1. Chronic Renal Failure GONAH + skin + neuro + GIT Concise Long Case Approach Growth (paeds) Height/ weight Osteodystrophy Bone pain History Fractures Arthritis Presenting complaint Proximal myopathy “I have renal failure” Nutrition Protein intake complications Water restriction (glomerular) or excess (interstitial) unrelated problem Electrolytes Anemia Pallor, lethargy, fatigue Past history SOB first diagnosis when Hypertension treatment presenting complaint Skin Sallow o enquire about urinary symptoms Pruritis frothy urine GIT NVD 0 hematuria Neuro Seizures – 2 electrolyte disturbances oliguria/anuria/polyuria/nocturia Encephalopathy Peripheral neuropathy etiology: Complications of treatment Commonest Other Dialysis – bleeding/ infections/ occlusion DM Renal Immunosuppressive drugs – cyclosporine/ azothioprine/ prednisolone ask for past history Renovascular ask for polyuria/polydipsia/polyphagia Interstitial nephritis e.g. drugs Functional – days off work/school, change of job, financial HTN Cystic kidney diseases – family history The standard remaining history ask NSAIDs—analgesic nephropathy GN Pyelonephritis e.g. told of kidney VITAMIN infection? Fever? Physical examination Vascular – HSP – rashes/joint/abdpain Stones – loin to groin pain, previous Infectious – strep sore throat/ HBV stones General Ht/Wt Toxin – gold/ penicillamine Anatomical – e.g. VUR, BPH Cachexia Autoimmune – SLE symptoms o Myoclonus 2 uremia Metabolic – DM Extrarenal o 0 Cusingoid appearance 2 steroids 1 causes SLE Skin Sallow systemic sclerosis Scratch marks myeloma Hands/ Arms Asterixis Leuconychia Investigations done Lindsay’s ½ and ½ nails (proximal white distal brown) U/S – anatomical malformations Palmar crease pallor Biopsy - GN AV fistula – thrill present is important sign of patency Myopathy Management medications Face/ chest Fundoscopy – HTN/DM changes dialysis Anemia AV grafts Central line Transplant/ waiting list? Tanner Staging Rickety rosary ribs Disease progression and Complications of disease Heart Pericardial rub CCF DO YOU STILL PASS URINE NOW? (GIVES AN ESTIMATION OF SEVERITY OF Bruit suggest vascular cause of CRF RENAL FAILURE) Lungs Creps
- 2. Abdomen Nephrectomy scar – usu. postero-lateral Management Transplant scar (usu iliac fossa) and transplant kidney Kidneys ballotable, bruit Growth failure Treat all contributors to growth failure Bladder Malnutrition – inadequate protein Enlarged prostate Anemia Legs Edema Osteodystrophy Neuropathy GH resistance PVD Genu varum If ht<3%, velocity<50%, give rHGH tx Other Bone and joint tenderness Osteodystrophy Low phosphate diet (eg avoid diary products) BP Phosphate binders (CaCO3, Ca acetate) Calcium supplements (CaCO3, Ca acetate) Manifestations of DM, HTN, SLE Vitamin D supplementation Nutritional If HD/PD, give recommended daily allowance + additional protein to compensate for losses from dialysis Investigations Fluid – fluid restriction in ESRF and fluid overload type CRF to confirm diagnosis of CRF (eg 500ml/day, keep wt gain to <1kg/day), if salt-losing type to determine etiology of CRF CRF, encourage H20 intake to look for complications of CRF Na 2g/d K usu well maintained, treat as emergency if hyperK Diagnosis & U/E/Cr Creatinine to estimate GFR Ca gluconate staging By MDRD study equation Insulin + dextrose By Cockcroft-Gault formula Salbutamol Etiology Bloods Plasma glucose Resin (Ca Resonium) ASOT/ HBV/ ANA/ C3 Dialysis Urine Urinalysis Low phosphate diet 800mg/day Radiology Renal U/S – cysts Anemia Causes of Anemia IVU – Stones Decreased EPO synthesis MCU – if suspect anatomical abnormalities in Shortened RBC survival due to uremia paeds Management DMSA/ DTPA Adequate dialysis Biopsy GN Keep >10g% Complications Bloods FBC – Anemia Do Fe studies (Fe, ferretin, transferring, TIBC) Serum – Ca/ PO4/ ALP/ PTH rEPO if not Fe-deficient U/E/Cr – electrolyte imbalance Hypertension ACE-inhibitor Radiology CXR – heart/lungs Ca++ blocker Bone Xrays Neurological Electrolyte control Stages of CKD (based on KDOQI guidelines from the National Kidney Foundation) 2 Stage GRF (ml/min/1.73m ) 1 ≥90 2 60-89 3 30-59 4 15-29 5 = ESRD <15
- 3. Issues: CKD Vit D products (eg calcitriol) A) Ca/PO4 metabolism in CKD - give if iPTH >21 or 3x normal upper limit - contraindications: Ca- PO4 >55, PO4 >2.0 or iPTH <15 (as further suppression of iPTH by Vit D will cause impaired bone remodeling and higher risk of fractures Decreased renal Decreased Acidosis secondary to - monitoring of iPTH – ideally, yearly in stage 3, half yrly in stage 4, 4-6 mthly in stage 5 excretion of PO4 renal mass + decreased H excretion 4) Secondary hyperparathyroidism due to hyperplasia of parathyroid gland iPTH usually >100 perform U/S or Sestamibi scan to locate PTH glds, as there may be >4. Sestamibi scan preferred Decreased Rx: surgical removal +/- partial reimplantation of portion of PTH gland hydroxylation of Vit D 5) Treating hypocalcaemia Decreased GI IV Ca Gluconate contains 2.4mmol/10ml, IV CaCl2 contains 7 mmol/10ml of calcium Ca absorption ions Higher risk of phlebitis with CaCl2, and also, more severe in event of extravasation. Always give CaCl2 intra-hemodialysis, via central line, or at least via large bore cannula Decreased if possible, unless in event of emergency. serum Ca Increased bone B) Anaemia in CKD Increased iPTH osteoclastic activity Causes LVH and increase risk of cardiovascular disease secretion Ideal target 11-11.5 g/dL, however locally, usually aim for 8g/dL in view of Rx costs. (Note: Hb > 12.5 also a/w increased mortality) iPTH/PO4 Work up: iPTH and PO4 levels start rising o Fe panel – Ferritin <200 + Tsat <20% = Fe deficiency in hemodialysis exponentially from CKD stage 3 (in peritoneal dialysis, limit for ferritin is <100) increased PO4 levels correlates to greater Tsat = transferrin saturation = Fe ÷ transferring x100% cardiovascular risk o Vit B12/folate o PBF o OGD o +/- stool OB Mx 1 2 3 4 5 Mx 1) Diet – first line Fe Fumarate – 400-800mg/day, give on empty stomach (eg ON) - limit PO4 intake to 800mg/day (dietician r/v) IV venofer 100mg x 8-10 doses. CI: Ferritin >500 or Tsat >50% 2) Phosphate binders Erythropoeitin i) CaCO3 - higher elemental Ca load, & better tasting. Therefore better for o Start if Hb <10-11. Starting dose 100unit/kg/wk (eg 6000U/wk). calcium supplementation Monitor for 3-4 wks before increasing dose as necessary. ii) Ca Acetate – higher phosphate binding capacity, but large and bad tasting. o Max 30,000 U/wk Better for managing high phosphate levels o If poor response, consider possible causes iii) MgSO4 – bad tasting, risk of Mg toxicity. Common SE of diarrhea Inflammation/infection (raised ferritin) iv) Al(OH)3 – risk of aluminium toxicity (eg poor BP ctrl, encephalopathy), not for Malnutrition (low albumin) use for >6wks. Secondary hyperparathyroidism v) Seralamer – amino acid polymer. Gd for ctrl of acidosis as well, but expensive Malignancy vi) Dialysis Aluminium toxicity Give CaCO3/ Ca acetate between meals if trying to supplement Ca. Give with meals if ACE/ARB trying to bind phosphate. Insufficient dialysis Calcium-phosphate binding product = [Ca] x [PO4] Pure red cell aplasia (rare) - if >55 (calculations in mmol), OR if [Ca] 2.50 mmol/L, avoid Ca based phosphate binders in view of risk of metastatic calcium product deposition Targets: CKD Stage 3-4 keep [PO4] <1.5; Stage 5 keep [PO4] <1.8 Low phosphate levels also indicate likely malnutrition, as PO4 is found in high protein Digitally signed by DR WANA HLA SHWE DN: cn=DR WANA HLA SHWE, c=MY, food o=UCSI University, School of Medicine, KT- Campus, Terengganu, ou=Internal Medicine 3) Calcium supplementation Group, email=wunna.hlashwe@gmail.com Reason: This document is for UCSI year 4 CaCO3/ Ca acetate between meals students. Date: 2009.02.22 15:45:33 +08'00'
- 4. CHRONIC RENAL FAILURE WITH FLUID OVERLOAD – PATHWAY Treatment Orders: 1. Diuresis with IV frusemide: Investigations: 120-240 mg/8hrly (if serum Cr > 400 μmol/L) • FBC--anaemia 80-120 mg/8hrly (if serum Cr < 400μmol/L) • PT/PTT, GXM—for dialysis, transfusion If no response, step up to maximum OR infusion at 30 mg/hr • U/E/Cr/HCO3/Glucose—renal fxn, DM Urinary catheter if no urine output > 6hrs • HbA1c if diabetic--DM • Ca/Phosphate/Magnesium—renal osteodystrophy 2. Exclude cardiac event • Fasting iPTH—endocrine compx Check baseline ECG • LFT If pt has IHD, do CK/CKMB/Trop T Repeat ECG x3 • Fasting lipids--hyperlipidaemia • ECG/CXR ) 3. Consider acute dialysis/filtration (if hypoxic, severe fluid overload, acidosis, or • ABG on room air—metab acidosis ) exclude AMI hyperkalaemia) • CK/CKMB ) PT/PTT, GXM • UFEME, Urine c/s If for dialysis, trace Hep/HIV status. If results > 6mths, order HBsAg, Anti-HCV, HIV Day 2: 4. (Day 3) If anaemia workup negative, consider erythropoietin therapy – refer • If Hb<11 g/dL: pharmacist and inform on cost Fe/TIBC Ferritin 5. (Day 5) Review CXR: if clear, consider switching to oral frusemide. If well on oral B12 / folate frusemide, consider discharge Stool OB x3 • If Hb<6 g/dL 6. Discharge plan: Consider OGD, transfusion, thal workup etc Fluid restriction Nutritional restriction (decreased protein, potassium, phosphate, calories (if DM)) Nutrition: When to seek medical help: skin turgor, pitting oedema, weakness, fatigue, • Low salt muscle cramps, N/V • Low protein 0.8g/kg/day Skin care • Low phosphate Identify primary physician, appointments, home care etc. • Low potassium • DM 1500/1800/2000 kcal Referral Plan (Day 2 onwards): • If Cr > 400 μmol/L Fluids: Assess ADL (toilet needs, dressing, feeding) • 500ml/day (if serum Cr > 400 μmol/L) If can’t do any one ADL, refer MSW • 800ml/day (if serum Cr < 400μmol/L) If can do all, refer renal coordinator, vascular surgeon • If Cr < 400 μmol/L, refer renal coordinator, MSW, vascular surgeon as required • Others: pharmacist, physiotherapist, psychologist etc. Assessment: • Vital signs • Height/weight • Urine dipstick • Pruritus • Oedema – sites and severity Digitally signed by DR WANA HLA • Compliance with fluid restriction SHWE • I/O charting DN: cn=DR WANA HLA SHWE, c=MY, o=UCSI University, School of Medicine, • IV plug KT-Campus, Terengganu, ou=Internal • O2 therapy Medicine Group, email=wunna. hlashwe@gmail.com • Urinary catheter if required Reason: This document is for UCSI year 4 students. Date: 2009.02.22 15:43:25 +08'00'