1. Nephrotic Syndrome Complications of Nephrotic Syndrome
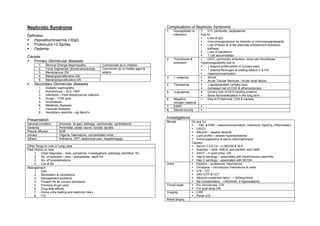
1. Susceptibility to UTI, peritonitis, septicaemia
Definition infections Due to:-
Loss of IgG
Hypoalbuminaemia <30g/L Immunosuppression by steroids or immunosuppressants
Proteinuria >3.5g/day Lost of factor B of the alternate complement activation
Oedema pathway
Loss of transferrin
Causes T cell abnormalities
2. Thrombosis & DIVC, pulmonary embolism, renal vein thrombosis
Primary Glomerular diseases embolism Hypercoagulability due to
1. Minimal Change Nephropathy Commonest dx in children ↓ plasma antithrombin III (urinary loss)
2. Focal Segmental Glomerulosclerosis Commoner dx in middle-aged & ↑ plasma fibrinogen & clotting factors V & VIII
3. Membranous GN elderly Haemoconcentration
4. Mesangioproliferative GN 3. ↓ volaemia Shock
5. Membranoproliferative GN Acute Tubular Necrosis / Acute renal failure
Secondary Glomerular diseases 4. ↑lipidaemia ↓ apolipoprotein (urinary loss)
1. Diabetic nephropathy increased risk of CHD & atherosclerosis
2. Autoimmune – SLE, HSP 5. ↓calcaemia Urinary loss of Vit D binding proteins
3. Infections – Post-streptococcal infection Bone demineralization in the long term
4. Drugs – TCM, gold 6. Negative Due to Proteinuria, LOA & nausea
5. Amyloidosis nitrogen balance
6. Metabolic diseases 7. ESRF
7. Vascular diseases 8. Steroid toxicity
8. Hereditary nephritis – eg Alport’s
Investigations
Presentation Bloods Dx and Cx:
General condition Anorexia, wt gain, lethargy, xanthomata, xanthelasma FBC & ESR – haemoconcentration, infections, hypoCa, inflammation
Oedema Periorbital, pedal, sacral, scrotal, ascites U/E/Cr
Pleural effusion SOB Albumin – assess severity
Urinary Oliguria, haematuria, concentrated urine Lipid profile – assess hyperlipidaemia
Others Infections, HPT, abdominal pain, hepatomegaly Immunoglobulins & serum electrophoresis
Causes:
Other things to note in Long case Serum C3 & C4 – in MCGN & SLE
Past History to note AutoAbs – ANA, ANCA, anti-dsDNA, anti-GBM
1. Initial diagnosis – date, symptoms, investigations, aetiology identified, Rx ASOT – in post-strep. GN
2. No. of episodes / year – precipitants, usual Rx Hep B serology – associated with membranous nephritits
3. No. of hospitalizations Hep C serology – associated with MCGN
4. Cxs & Mx Urine Dipstick – proteinuria, haematuria
Management Urinalysis – microscopic haematuria & casts
1. Diet C/S – UTI
2. Medication & compliance 24hr UTP & CCT
3. Management problems Albumin:creatinine ration - > 200mg/mmol
4. Present Rx for current admission Na Concentration - <20mmol/L if hypovolaemic
5. Previous drugs used Throat swab For microscopy, C/S.
6. Drug side effects For post-strep GN
7. Home urine testing and nephrotic diary Imaging CXR
8. F/U Renal U/S
Renal biopsy
2. Management
1. Bed rest, monitoring U/E, BP, fluid I/O charting, weight
2. Fluid restriction 1-1.5L/day
salt restriction
high protein diet
3. Diuretics Frusemide 80-250 mg PO ± spironolactone
Aim for loss of 1kg/day
Occasionally high dose frusemide + IV salt-poor albumin to
promote diuresis. However, risk of renal failure secondary to
hypovolaemia with over diuresis
4. Chronic nephrotic Consider reducing proteinuria with ACEI or cyclosporine
syndrome
5. Hyperlipidaemia Consider statin.
Usually improves with resolution of nephrotic syndrome
6. Hypertension Conventional regimens
7. Anticoagulation Prophylactic heparin for immobile PTs
Warfarin for symptomatic thrombosis
8. Infections Prophylactic ABx
Pneumococcal vaccination during remission
9. Mx of minimal change High dose corticosteroids
nephropathy in ± cyclophosphamide / cyclosporine in steroid dependant NS
children
Digitally signed by DR WANA HLA SHWE
DN: cn=DR WANA HLA SHWE, c=MY,
o=UCSI University, School of Medicine, KT-
Campus, Terengganu, ou=Internal Medicine
Group, email=wunna.hlashwe@gmail.com
Reason: This document is for UCSI year 4
students.
Date: 2009.02.24 10:17:10 +08'00'