More Related Content
Similar to Scleroderma long case summary
Similar to Scleroderma long case summary (20)
Scleroderma long case summary
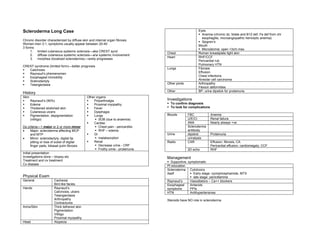
- 1. Scleroderma Long Case Eyes
Anemia (chronic dz, folate and B12 def, Fe def from chr
esophagitis, microangiopathic hemolytic anemia)
Chronic disorder characterized by diffuse skin and internal organ fibrosis Sjogren’s
Women:men 3:1, symptoms usually appear between 20-40 Mouth
3 forms: Microstomia: open <3cm max
1. limited cutaneous systemic sclerosis—aka CREST synd
Chest Roman breastplate tight skin
2. diffuse cutaneous systemic sclerosis—a/w systemic involvement
Heart RHF/CCF
3. morphea (localized scleroderma)—rarely progresses
Pericardial rub
Pulmonary HTN
CREST syndrome (limited form)—better prognosis
Calcinosis Lungs Fibrosis
Raynaud’s phemenomen Effusion
Esophageal immobility Chest infections
Sclerodactyly Alveolar cell carcinoma
Telangectasia Other joints Arthropathy
Flexion deformities
Other BP, urine dipstick for proteinuria
History
Skin Other organs
Raynaud’s (90%) Polyarthralgia Investigations
Edema Proximal myopathy To confirm diagnosis
Thickened stretched skin Fever To look for complications
Cutaneous ulcers Dysphagia
Pigmentation, depigmentation Lungs Bloods FBC Anemia
(vitiligo) SOB (due to anaemia) U/E/Cr Renal failure
Cardiac ANA Nearly always +ve
Dx criteria—1 major or 2 or more minor Chest pain - pericarditis Scleroderma
• Major: scleroderma affecting MCP RHF – edema antibody
and MTP GI Urine dipstick Proteinuria
• Minor: sclerodactyly, digital tip malabsorption urinalysis
pitting or loss of subst of digital Renal Radio CXR Effusion, fibrosis, CA
finger pads, bibasal pulm fibrosis Decrease urine - CRF Pericardial effusion, cardiomegaly, CCF
Frothy urine - proteinuria 2D echo RHF
Initial presentation
Investigations done – biopsy etc Management
Treatment and cx treatment Supportive, symptomatic
Cx disease
Pt education
Scleroderma Cytotoxics
itself Early stage: cyclophosphamide, MTX
Physical Exam late stage: penicillamine
General Cachexia Raynaud’s Vasodilators – Ca++ blockers
Bird like facies Esophageal Antacids
Hands Raynaud’s symptoms PPIs
Calcinosis, ulcers HTN Antihypertensives
Telangiectasia
Arthropathy Steroids have NO role in scleroderma Digitally signed by DR WANA HLA
Contractures SHWE
Arms/Skin Thick tethered skin DN: cn=DR WANA HLA SHWE,
Pigmentation c=MY, o=UCSI University, School of
Medicine, KT-Campus, Terengganu,
Vitiligo ou=Internal Medicine Group,
Proximal myopathy email=wunna.hlashwe@gmail.com
Reason: This document is for UCSI
Head Alopecia year 4 students.
Date: 2009.02.22 15:19:28 +08'00'