SASH : Lymphoma by Dr Veronika Langova & Dr Sophia Tzannes
•Download as PPT, PDF•
2 likes•3,260 views

Lymphoma by Veronika Langova. Veterinary consultancy content from SASH.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (19)
Similar to SASH : Lymphoma by Dr Veronika Langova & Dr Sophia Tzannes
Similar to SASH : Lymphoma by Dr Veronika Langova & Dr Sophia Tzannes (20)
Recently uploaded
Recently uploaded (20)
SASH : Lymphoma by Dr Veronika Langova & Dr Sophia Tzannes
- 1. Personalized lymphoma treatment Small Animal Specialist Hospital Dr Veronika Langova & Dr Sophia Tzannes
- 2. Personalized lymphoma treatment • LSA is the most common hematolymphatic neoplasm accounting for 5 % of all canine malignancies • Annual incidence 1/4000 dogs • Most dogs present w generalized lymphadenomegaly • Most dogs have high grade LSA w small proportion of having low grade or indolent form
- 3. Personalized lymphoma treatment • Aim of this talk is to alert you to the less commonly seen types of LSA which require recognition and appropriate management • Questions: • How do we diagnose them? • What is the clinical relevance?
- 4. Personalized lymphoma treatment • Treatment of hematopoetic neoplasia requires a specific, rather than general diagnosis that is based on cell architecture, cell morphology, phenotype and genetic rearrangement
- 5. Lymphoma classificationLymphoma classification • Changes in our understanding of lymphoid neoplasms have resulted in the evolution of numerous clinical and pathologic classification schemes over the past 50 years. • In 1994, the Revised European-American Lymphoma (REAL) classification was proposed which incorporated morphologic, immunophenotypic, genotypic and clinical features into disease subtype definitions.
- 6. Lymphoma classificationLymphoma classification • In 2001, the World Health Organization (WHO) introduced a new classification built on the REAL classification that represents the current “gold standard” for classifying all human hematopoietic neoplasm’s. • This classification provides system ofThis classification provides system of categorizing lymphoid neoplasm according tocategorizing lymphoid neoplasm according to their level of cellular maturation that alsotheir level of cellular maturation that also provides a level of prognostic indicationprovides a level of prognostic indication
- 7. Classifying canine lymphomasClassifying canine lymphomas • Valli et al produced a paper in 2010 which looked at the accuracy and consistency of veterinary pathologists in applying the WHO system of classification to canine lymphomas. This study found that veterinary pathologists could achieve a high degree of accuracy in applying the WHO classification system to canine lymphomas. • Since only follicular lymphoma can be accurately diagnosed on H&E staining and that subtype is uncommon, immunophenotyping is essential for an accurate diagnosis of canine lymphoma. • All cases were phenotyped w CD3/CD79, if histiocytic proliferation was present then CD18 was tested • Clonality was verified with PCRClonality was verified with PCR • Genetic rearrangement was evaluatedGenetic rearrangement was evaluated
- 8. Classifying canine lymphomasClassifying canine lymphomas• Summary of Canine Malignant Lymphoma Revised From the Revised European-American Classification of Lymphoid Neoplasms/ World Health Organization Classification of Lymphoid Neoplasms B Cell Neoplasms Precursor B cell neoplasms Precursor B lymphoblastic leukemia/lymphoma Mature (peripheral) B cell neoplasms B cell chronic lymphocytic leukemia/prolymphocytic Leukemia/small lymphocytic lymphoma B cell prolymphocytic leukemia Lymphoplasmacytic lymphoma Splenic marginal zone B cell lymphoma Plasma cell myeloma/plasmacytoma Extranodal marginal zone B cell lymphoma of mucosa-associated lymphoid tissue type Nodal marginal zone lymphoma Follicular lymphoma Mantle cell lymphoma Diffuse large B cell lymphomaa Mediastinal large B cell lymphoma Burkitt’s lymphoma/Burkitt’s cell leukemia Provisional entity: high-grade B cell lymphoma Burkitt’s-likea Primary effusion lymphoma T Cell and Putative Natural Killer Cell Neoplasms Precursor T cell neoplasm Precursor T lymphoblastic Lymphoma/leukemia Mature (peripheral) T cell and natural killer cell neoplasms T cell prolymphocytic leukemia Large granular lymphocyte leukemia (LGL) Aggressive natural killer (NK) cell leukemia Peripheral T cell lymphomas, unspecifieda Adult T cell lymphoma/leukemia Intestinal T cell lymphoma (+enteropathy associated) Hepatosplenic gdT cell lymphoma Subcutaneous panniculitis-like T cell lymphoma Mycosis fungoides/Sezary syndrome Anaplastic large cell lymphoma, T and null cell primary cutaneous type Peripheral T cell lymphoma not otherwise specified Angioimmunoblastic T cell lymphoma Angiocentric T cell lymphoma a Peripheral T cell lymphomas are those that are not otherwise specified (NOS) to a specific subtype by further definition
- 9. • 7 diagnostic categories then divided into 3 major groups ; – high, intermediate, low • Most common LSA centroblastic large B cell • Longest survival low-grade T cell (T-zone ) 622 days • Shortest survival T cell high grade (peripheral T cell) 162 days • high grade LSAs –unwell • • indolent low grade –free of CS ValliValli et alet al
- 10. • LSA is generally extremely sensitive to chemotherapy w CR 65-90% MST 26-51 W • Variety of chemo protocols are used and general consensus is that Doxorubicin – containing protocols are associated with the longest DFI and OS • Does specific diagnosis of LSA subtype have a similar impact on ST in dogs as it did in humans and did specific diagnosis in a dog impelled the specific chemotherapy required? • Effect of Tx chemotherapy for high grade B and T cell LSA inc ST • Contrary chemotherapy for T zone LSA decreased ST ( 13 dogs no Tx longest ST 687D0 • ValliValli et alet al
- 11. ImmunophenotypingImmunophenotyping • Immunohistochemistry and immunocytochemistry refer to the process of detecting antigens in tissues or cells by exploiting the antigen-antibody binding process found in biological tissues.
- 12. ImmunophenotypingImmunophenotyping • The diversity of immunophenotyping markers used in diagnostic pathology is substantial and more markers are becoming available in the veterinary field. Some examples of commonly used markers include: – CD3: T cell lymphoma – CD79a: B cell lymphoma – CD18, 11: Histiocytic disease – CD117: KIT used to identify MCT’s and GIST’s – Vimentin: a marker common to sarcomas
- 13. ImmunophenotypingImmunophenotyping • Histologic and immunohistochemical review of splenic fibrohistiocytic nodules (SFHN) in dogs Moore 2012 – Splenic FHN cases were re-evaluated in 32 dogs – Histo Grade I(2) Grade II (9) Grade III(21) dogs – CD3,CD20,CD79a,CD18,CD11d, K1-67 used to reclassify – Grade I- MZL and lymphoid nodular hyperplasia – Grade II-MZ hyperplasia(1), MZL (1), complex hyperplasia (2), LNH(1), stromal sarcoma (3) – Grade III- MZH(1), diffuse large B cell LSA(1), MZL(1)CNH (6),LNH (1), SS (5), HS (6) – Prognosis HS- poor 74 days • stromal sarcoma 488 days, 565 alive 1 year • 8 dogs with CNH MST 387 D 70% alive 1 year • 5 dogs with LNH MST 570 D 60% alive 2 years post splenectomy
- 14. PARR and FlowPARR and Flow• What is the difference between flow cytometry and PARR? • The PARR assay is a PCR assay in which we are amplifying DNA to evaluate lymphocyte (LCT) receptor gene length. In a heterogenous LCT population the LCT’s are all genetically distinct so the LCT receptor genes vary in length. • Homogenous or clonal LCT population, is often malignant and have identical gene length throughout the population. • • The results tell us if the majority of cells in the sample are derived from the same original clone (most consistent with neoplasia), or from multiple clones (most consistent with a reactive process- inflammation, immune mediated dz or infection)
- 15. PARR and FlowPARR and Flow • What is the difference between flow cytometry and PARR? • Flow cytometry (FC) allows identification and quantitation of cell surface markers • The FC study involves staining live cells (blood, BM, LCT) with labelled antibodies that bind to proteins expressed on the cell surface • The cells are analyzed on a flow cytometer, which tells us how many cells of each type are present. This information allows us to determine the lineage of the cells present, and whether they are homogeneous (more consistent with neoplasia) or heterogeneous (more consistent with a reactive process • Limitation – sample collection- EDTA, 24 hours not frozenLimitation – sample collection- EDTA, 24 hours not frozen
- 16. Ben 10yr MN JRT • Presented November 2012 with haemabdomen • Splenectomy was performed •
- 17. HISTOPATHOLOGY REPORT An 80mm coarsely multinodular portion of dark semi-firm tissue. On section, the cut surface presents multiple 1- 3mm diameter multifocal coalescing pale foci, sometimes with central congestion or haemorrhage. Multiple representative sections (A-J) are taken. GROSS PATHOLOGY The pale foci evident on macroscopic examination correspond to irregular coalescing multinodular aggregations of marginal zone-type monocytoid lymphocytes. The aggregations are centred on the arteriolar structure of the spleen. The monocytoid lymphocytes infiltrate the walls of blood vessels and there is subendothelial colonisation by neoplastic cells. The mitotic index approximates 2 mitoses per 10 high-power fields. Residual splenic tissue is congested and has infiltration by haemopoietic cells. DIAGNOSIS: Lymphoma COMMENTS: This is a low to moderate grade large-cell type of lymphoma originating probably from follicular marginal zone lymphocytes (MZL). Marginal zone lymphomas are usually indolent. Ben 10yr MN JRT
- 18. Indolent lymphoma in humansIndolent lymphoma in humans • If detected early and only involving one or two lymph nodes, radiation is often recommended and this can result in a cure or long- term remission. • A ‘watch and wait’ approach is commonly undertaken patients are asymptomatic • Traditionally fairly chemo- RT resistant- conservative Tx recommended • The clinical course is extremely variable, with some patients having an extremely aggressive course and death within 1 year, whereas others may live for more than 20 years and never require therapy. • Disease transformation to a more aggressive histologic type is a common terminal event • Most patients are >60yrs of age and present in an advanced state of disease with >50% having bone marrow involvement
- 19. Indolent lymphoma in dogsIndolent lymphoma in dogs • Indolent lymphoma comprises 5- 29% of all canine lymphomas • Limited information regarding the subtypes and biological behavior. • Canine indolent lymphoma consists of a group of diseases that are histopathologically similar to subtypes of non-Hodgkin’s lymphoma identified in people. • Histopathological subtypes: • B cell- marginal zone (MZL), follicular lymphoma • (FL) and mantle cell lymphoma (MCL ), • T-zone lymphoma (TZL).
- 20. 20 Germinal centre of follicle Marginal zone Lighter Trabeculae Capsule Mantle zone Darker
- 21. Indolent lymphomaIndolent lymphoma • B cell predominant • Both B and T cell indolent lymphomas share a low mitotic rate, slow rate of progression • TZL can be difficult to recognize as malignancy given the small mature –appearing cell type and low mitotic activity. • Detection of clonality is useful adjunct to histologic examination
- 22. Indolent lymphomaIndolent lymphoma • Splenic marginal zone lymphoma in 5 dogs - Stefanello et al 2011 • small study, retrospective • Hallmark of splenic MZL was focal hypoechoic mass, which became symptomatic only if ruptured. • Unlike in Hu BM involvement is rare 0/5 • ST- 760,939, 1825 days, one alive 445 days, one died 180 days.
- 23. Indolent lymphomaIndolent lymphoma • Clinical characteristics and outcome in dogs with splenic Marginal Zone LSA O’Brien JVIM 2013 • 34 dogs retrospective study • MZL – nodal, splenic, mucosa associated • Little known about clinical outcome • CS - 15/29 attributed to splenic MZL - hemoabdomen, distended abdo, lethargy, anorexia + weight loss • Only 1 dog with disseminated dz, rest were splenic only • Pre-sx dx - FNA of spleen 13/29 dogs, + result in only 3, 10 - extramedullary hematopoiesis, hyperplasia, reactive, inconclusive
- 24. Indolent lymphomaIndolent lymphoma • Clinical characteristics and outcome in dogs with splenic Marginal Zone LSA O’Brien JVIM 2013 • Good outcome after splenectomy overall MST 383D, 571 days with exclusion of perioperative deaths. • Only 5 dogs did not have any other concurrent disease - MST 1001dOnly 5 dogs did not have any other concurrent disease - MST 1001d • Only PF was diagnosing MZL as incidental finding • Chemotherapy may not increase ST= human counterpart, chemo used only if splenectomy is contraindicated. • Chemotherapy can select for more aggressive behavior in indolent LSA
- 25. So how is Ben? •
- 26. Piper Rossano 11yr FS Labrador • Presented with pancytopaenia and • splenomegaly. • No peripheral lymphadenopathy • Ultrasound guided splenic FNA • The liver was aspirated and bone marrow collected.
- 27. Piper Rossano 11yr FS Lab • HAEMATOLOGY • Test Result Alert Units Reference Range • *RBC 3.2 Low x10^12/L 4.9 - 8.2 • *HAEMOGLOBIN 66 Low g/L 100 - 206 • *HAEMATOCRIT 0.20 Low L/L 0.35 - 0.58 • *RETICULOCYTE % 3.8 High % 0.0 - 1.5 • *RETICULOCYTE ABS 122 High x10^9/L 10 - 110 • *MCV 63 Low fL 64 - 76 • *MCH 21 pg 21 - 26 • *MCHC 330 g/L 310 - 360 • *PLATELETS Decreased • *PLATELET COUNT 63 Low x10^9/L 200 - 500 • *WBC 3.5 Low x10^9/L 4.5 - 17.0 • *NEUTROPHILS% 74 % • *NEUTROPHILS 2.6 Low x10^9/L 3.5 - 12.0 • *LYMPHOCYTES% 9 % *EOSINOPHILS 0.0 x10^9/L 0.0 - 1.4 *BASOPHILS% 0 % *BASOPHILS 0.0 x10^9/L *PROTEIN PLASMA 56 Low g/L 62 - 85 *PLASMA APPEARANCE Normal *BLOOD SMEAR EXAMINATION Moderate anisocytosis Mild macrocytosis White cell morphology normal.
- 28. Piper Rossano 11yr FS Labrador• SPLENIC ASPIRATE; Four routinely stained slides • DESCRIPTION: Four slides of high cellularity and excellent quality are examined. Slides contain many neoplastic round cells and few haematopoietic progenitors present both within and between moderate numbers of splenic stromal fragments and abundant blood. • Neoplastic round cells are large (15-25um in diameter), moderately pleomorphic, present individualised, and discrete. Nuclei are round to rarely reniform in shape and eccentrically located with finely granular chromatin containing 1-4, often prominent, nucleoli. Cytoplasm is scant to moderate in amount, deeply basophilic, often vacuolated, and occasionally contains erythrocytes. Mitoses are occasionally noted. Pleomorphism is characterised by moderate anisocytosis, moderate anisokaryosis, multiple nucleoli, and occasional reniform nuclear shapes. • Haematopoeitic progenitors are most often erythroid with few myeloid and rare megakaryocytes. No microorganisms are noted. • INTERPRETATION: Malignant round cell neoplasia; Probable lymphoproliferative disease (see comment) • COMMENTS: The predominant cellular population is the neoplastic round cells. These are most cytologically compatible with lymphoid cells and as such large cell/anaplastic lymphoma or acute lymphoid leukaemia (ALL) are the most likely differentials. Acute lymphoid leukaemia must be considered given the pancytopenia although no circulating neoplastic cells were noted on review of the blood smear. • The moderate pleomorphism, occasional reniform nuclear shapes, moderate amounts of cytoplasm, and occasional erythrophagocytosis allow for histiocytic sarcoma as a less likely differential. So, consider confirming lymphoproliferative disease with immunocytochemistry or PARR (on splenic aspirate slides or bone marrow aspirate slides if the cells are present within the bone marrow) or biopsy of an abnormal organ (eg spleen or any lymph nodes that are enlarged) with immunohistochemistry. Bone marrow aspirate would be recommended to evaluate for leukaemia as this is a poor prognostic indicator. • LIVER COMMENTS: The neoplastic cells within the liver are the same as the neoplastic cells present within the spleen (4000073493) and again are interpreted as most compatible with a large cell or anaplastic lymphoid population;
- 29. Piper Rossano 11yr FS Lab • Immunocytochemistry performed • and final diagnosis was T cell • hepatosplenic lymphoma • Treated with chemotherapy for 4 months and then showed signs of progressive splenic disease and abdominal discomfort.
- 30. Hepatosplenic lymphomaHepatosplenic lymphoma • Hepatosplenic lymphoma is a rare type of T cell lymphoma that is characterised by splenic, hepatic and bone marrow infiltration without peripheral lymphadenopathy • This is an aggressive type of lymphoma with patients presenting with cytopaenia’s and hypoproteinemia • Hepatocytotropic T cell LSA- not only hepatic sinusoids but invasion of hepatic cords (CD11d-) • In humans, this disease is more often seen in immunosuppressed patients (organ transplant recipients) and there has been a link to azathioprine • CHOP frequently induces remission but this disease is aggressive and prognosis is poor
- 31. Koira Livingstone 7yr F Spitz • Presented with vomiting and elevated liver enzymes (ALT 916, AST 168, ALP 331 GGT 32) • On initial ultrasound the liver parenchyma appeared normal • Treated symptomatically
- 32. Koira Livingstone 7yr F Spitz • Repeat ultrasound 1 week later again showed a slightly hypoechoic liver with enlarged hepatic lymph node and enzymes were still elevated • FNA’s of the liver/LN taken
- 33. 33 HEPATIC LYMPH NODE AND LIVER ASPIRATES; Ten routinely stained slides DESCRIPTION: The hepatic lymph node shows good cell recovery. Approximately 80% of cells are medium to large lymphoid cells with large round, eccentric nuclei and modest volumes of blue-grey cytoplasm. A juxtanuclear pale zone is evident in the cytoplasm of most cells. Together cell types include 13% small lymphocytes, 4% neutrophils, 1% plasma cells and 2% macrophages. Several large lymphoglandular bodies are evident in the background. The Liver shows islands of quite heavily vacuolated and swollen hepatocytes that are accompanied by large numbers of lymphoid cells. The majority of lymphoid cells are large, similar to those predominating in the lymph node aspirates. Much bile pigment and biliary casts are associated with the hepatocytes. COMMENTS: Lymphosarcoma of large lymphoid cells is evident in both the lymph node and liver. A vacuolar hepatopathy and cholestasis is also present Koira Livingstone 7yr F Spitz
- 34. 34 Koira Livingstone 7yr F Spitz • Immunocytochemistry diagnosed T cell lymphoma • Koira was started on LOPP chemotherapy in July 2013 and is still alive today! Koira Livingstone 7yr F Spitz
- 35. Snowy Dennett 11yr MN Devon Rex • Presented with a history of unilateral nasal discharge and sneezing • FIV positive • CT and rhinoscopy performed • after BP + coags were normal • Samples submitted for cytology • histology and bacterial/fungal • culture
- 36. • CT showed a soft tissue mass • occupying the left nasal cavit Snowy Dennett 11yr MN Devon Rex
- 37. • Macroscopic description: The specimen/s presented for examination are 10 pieces, 5- 8mm, cream-brown. • Microscopic description: Markedly expanding the nasal mucosa multifocally and destroying tissue architecture is a dense pleomorphic round cell proliferation. Nuclei are large, round or indented, and densely basophilic or finely stippled and nucleolated; cytoplasm is inconspicuous or scant and eosinophilic. Anisokaryosis is moderate and mitotic index is conservatively 12/10HPF. Individual cell apoptosis is frequent, there are larger areas of necrosis, haemorrhage and granulation tissue, and there is a variably mild to moderate infiltrate of neutrophils, small lymphocytes (including follicle formation), plasma cells and scattered macrophages. • Diagnosis: Nasal lymphosarcoma - large cell, high grade. • Comments: Sections show features of an aggressive round cell malignancy assessed as lymphosarcoma on the basis of cell morphology that includes little cytoplasm. Areas containing tumour are generally devoid of epithelium, presumably ulcerated; lymphocytic infiltration of epithelium elsewhere seems to be associated with reactive follicles rather than tumour. Additional changes are likely secondary to the tumour. IHC is available to further define the proliferation if necessary. Snowy Dennett 11yr MN Devon Rex
- 38. Feline lymphomaFeline lymphoma • Lymphoma is the most common neoplasm in cats, represented 30% of feline tumours. • It is associated with a bimodal age distribution, with a peak occurring at <4yrs and another at 8yrs of age. • Unlike canine lymphoma, which is typically multicentric involving peripheral lymph nodes, feline lymphoma has a variety of anatomic and histologic presentations.
- 39. Feline nasal lymphomaFeline nasal lymphoma • Seems to be Stage I disease • FeLV • 3 original reports using RT as primary Tx shown prolonged ST 40 months. • Response of 19 cats w nasal LSA to RT and chemotherapy Sfiligoi 2007 – Combination of RT 22-48 Gy with 6 months chemotherapy median PFI 31 months – 17/19 remission 10/17 remission all period of follow up, 4 local relapse, 3 distant dz – Negative PF- cribriform plate involvement • Survival analysis of 97 cats w nasal LSA Haney 2009 – RT, chemo and RT+chemo. MST 536 days – PF – anemia , + response to Tx and RT>32 Gy – Which RT protocol? Which chemo?
- 40. Feline lymphomaFeline lymphoma • Hodgking’s LSA cats • Hodgkin's lymphoma in humans is unique among lymphoid cancers in both its clinical and morphologic presentations. • In humans, Hodgkin's disease is described as a slowly progressive, even curable neoplasm of lymphoid tissue that arises in a single node or chain of nodes and spreads via contiguous nodes. Splenic and hepatic involvement succeed nodal disease, and only in the late stages of the disease is the marrow infiltrated.
- 41. Feline lymphomaFeline lymphoma • The disease presents histologically as a heterogeneous population of lymphoid and inflammatory cells with a minority of malignant Reed–Sternberg (RS) cells (and/or variants) scattered throughout the tissue.1,6 The presence of RS cells and their variants is not pathognomonic of the disease but is essential for a histopathologic diagnosis. • • Reed Sternberg cells Text Reed-Sternberg Cells
- 42. Feline lymphomaFeline lymphoma • The clinical presentation is unusual for feline lymphoma and appears very similar to that of human HD. • In 95% (19/20) of cases, the cats were presented with either a single enlarged lymph node (17/20) or two contiguous enlarged lymph nodes (2/20). •
- 43. Feline GI lymphomaFeline GI lymphoma • Increase incidence from 32% to 72.5% in post FeLV era • SI, stomach, mesenteric LNs and liver • Small cell LSA confined typically to GI tract • Low Grade GI LSA –T cell, high Grade B-cell • Large granular cell LSA – aggressive type of alimentary LSA, thought to be NK origin
- 44. Feline GI lymphomaFeline GI lymphoma • Why is diagnosis of alimentary LSA difficult? – Many reasons for infiltration of immune cells into SI in cat ( infections such as Mycobacteria, helicobacter, Giardia, Toxoplasma), chronic food allergies, idiopathic causes and enteric-associated T-cell infiltration are difficult to distinguish – Clonality and flow cytometry is useful • Small –cell LSA: – slow onset, chronic weight loss – Palpable ropey thickened intestines – 10% hypercalcemic – 78% low cobalamine levels – Tx Chlorambucil 15 mg/m2for 4 days q3 weeks – MST 704 days
- 45. Feline GI lymphomaFeline GI lymphoma • Large cell alimentary LSA – acute CS, 80% palpable abdominal mass, weight loss, obstruction and septic abdomen • Marked difference between small and large = diagnosis can be made on FNA – Prognosis is poor with MST 4-6 months RR 60% • Abdominal RT as rescue therapy 2011 Parshley – 11 cats, 2x8Gy response in 10/11 cats MST post RT 211 days
- 46. Before After Snowy Dennett 11yr MN Devon Rex
- 47. • Received COP chemotherapy • and re-staged once completed • which showed dramatic • improvement • Continued on maintenance • therapy and is still doing well • 12 months on Snowy Dennett 11yr MN Devon Rex
- 48. Forster Douglass 12yr MN Border Collie •Presented as a referral for a recurrent oral melanoma
- 49. 49 • Biopsy report: what are we expecting?Biopsy report: what are we expecting? • Options for dog?Options for dog? • a)a) Surgery and melanoma vaccineSurgery and melanoma vaccine • b) Radiation of massb) Radiation of mass • c) Carboplatin chemotherapyc) Carboplatin chemotherapy • d) Lomustine chemotherapyd) Lomustine chemotherapy • Further diagnosis with histopathology and immunohistochemistryFurther diagnosis with histopathology and immunohistochemistry Round cellsRound cells Histiocytic cells Mast cells Lymphoma Plasma TVT Epitheliotropic T cell lymphoma Amelanotic melanoma
- 50. 50 Lip mass. Extensively infiltrating through the submucosa are myriad round cells with scant amounts of lightly eosinophilic to clear cytoplasm and no obvious pigment. The cells have atypical lymphoid appearance with round nuclei containing granular to branched chromatin and 1 nucleolus. Some of the nuclei are indented while occasional cells have a slightly larger nucleus. The cells show aggregation around vessels as well as infiltration into bundles of nerve and skeletal muscle. The mitotic index is 5. There are scattered interstitial eosinophils, small dark lymphocytes, occasional plasma cells and macrophages. Within the overlying haired skin is a similar population of round cells showing epitheliotropism, and also affecting hair follicles, sebaceous glands and sweat glands. These cells often have clear cytoplasm and infiltrate epithelium as individual cells and small clusters. Affected regions of the epithelium are subtended by plasma cells, small dark lymphocytes and a few of the atypical lymphocytes. Distribution of this change within the affected haired skin is not uniform. The mucosal surface is affected but to a lesser extent. Neoplastic cells are not seen at mucosal and haired skin margins. IMMUNOHISTOCHEMISTRY REPORT The neoplastic lymphocytes within epithelium and deeper tissue are strongly and uniformly labelled with CD3 Epitheliotropic lymphomaEpitheliotropic lymphoma
- 51. 51 Epitheliotropic lymphomaEpitheliotropic lymphoma • Clinical presentation – Lesions clinically and histologically resemble many inflammatory skin diseases
- 52. 52
- 54. 54 Scott’s classification 1. Exfoliative erythroderma 2. Plaques/nodules 3. Ulcerative disease of oral mucosa 4. Mucocutaneous forms
- 55. 55 Comparative oncology: Mycosis fungoides – Mycosis fungoides = epitheliotropic T cell lymphoma • MF variants – Folliculotropic MF – Pagetoid Reticulosis (solitary form) (Woringer-Kolopp) – Granulomatous slack skin syndrome – Sezary Syndrome 5 year survival 88-100% 5 year survival 24% Patches and plaques <10% BSA >10% BSA T1 T2 1 + cutaneous tumour T3 Erythroderma T4
- 56. 56 Epitheliotropic lymphomaEpitheliotropic lymphoma Histopathology and ImmunohistochemistryHistopathology and Immunohistochemistry • IMHC: CD3 (CD8+) Photomicrograph (original magnification 400Å~) of a punch biopsy of skin from the preputial region of Rigby, stained with periodic acid-Schiff. Note evidence of invasion of epidermis and dermis by a monomorphic population of malignant lymphocytes (arrowhead) and epidermal microabscess (Pautrier’s microabscess) (arrow).
- 57. 57 Epitheliotropic lymphomaEpitheliotropic lymphoma DiagnosisDiagnosis • Histopathology – 50% (7/14) of oral cases were conclusively diagnosed with histopathology alone (Nemec et al, 2012) • early stages can have marked mixed inflammatory infiltrate, late stages > B lymphocytes • >50% there is a mix of lymphocyte cell size reported • IMHC – humans: 5-10% lymphoid neoplasia cannot be diagnosed with use of histopathology and IMHC • PARR – T cell receptor (TCR) gamma rearrangement – Sensitivity 80-95%, Specificity 96-100% Clinical features Histopathology Immunohistochemistry Clonality testing Clinical follow up and repeat biopsy
- 58. 58 • Thoracic radiographs, abdominal ultrasound, LN biopsy • Lomustine (CCNU) and prednisolone • Monitoring • Response: complete remission 7 months* – Lomustine ORR 78-83% (17-32% CR, 50-61% PR) – Median duration 88-94 days (Risbon et al, 2009, Williams et al, 2008) • Ionised hypercalcaemia noted at three months – Anal sac adenocarcinoma, surgery post staging – Melphalan and NSAIDS – Complete remission • ETL progressive disease at 7 months, despite recommencing lomustine • Euthanasia one week later due to ruptured splenic mass and haemabdomen Forster’s Epitheliotropic lymphomaForster’s Epitheliotropic lymphomaStaging and treatmentStaging and treatment Other therapies Surgery Radiation Retinoids Interferon Phototherapy Systemic chemotherapy Novel therapies
- 60. 60 New clinical trial • Brain tumours and Melanomas
- 61. 61 Drug Loading and Targeting
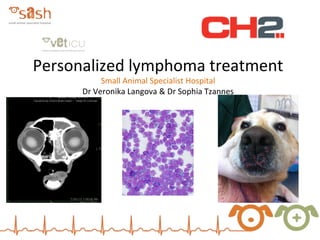
- 62. Axial sequential MRI scans showing brain tumor (white irregular mass) prior to EDV treatment Corresponding MRI scans showing almost complete elimination of tumor mass post-treatment with 5 doses of Canine EGFR EDVsDox
Editor's Notes
- infiltration of neoplastic T lymphocytes into skin with a specific tropism for epidermis and adnexal epithelium
- Marked variety of clinical presentation: patch- not raised/indurated, vs plaque is raised/indurated-can be assoc with ulceration; Differential diagnoses: sarcoptic mange, lupus erythematosus, pemphigus, drug reactions, food allergies skin scrapes and tapes, testing for hypothyroidism, blood work.... dxx incl sarcoptic mange, Zoetis scale and crust
- Image Vet Derm website
- 1. EE: &gt;80%, pruritis 40% 2. plaques/nodules 3.Ulcerative disease of oral mucosa (ulcerative stomatitis) 4.Mucocutaneous forms = 50% lips, nasal planum, eyelids, perianal junction, perivulvar junction) and oral cavity (buccal mucosa, gingiva, palate, tongue). Footpads and interdigital folds can be involved too. Depigmentation common Limitations of classification scheme: while this is helpful to be able to describe and ID the lesions, the majority of dogs present with multiple lesion types simultaneously. Disseminated disease often affects trunk, or is localised to head, esp around the nose. Limitations of classification scheme: while this is helpful to be able to describe and ID the lesions, the majority of dogs present with multiple lesion types simultaneously. In addition, different lesion types do not seem to have prognostic significance. This is in contrast to humans, where there is progression in stages: (scale&gt; patch&gt;plaque&gt;nodule/tumour), and these have prognostic implications.. For instance, diffuse erythema occurs in late stage disease in humans, and is a frequent (86%) and early finding in dogs. Also, we frequently see presence of tumour forms at onset in dogs, often in combination with other lesions, and this does not seem to affect prognosis.
- This is in contrast to humans, where there is progression in stages: (scale (psoriasis/eczema)&gt; patch&gt;plaque&gt;nodule/tumour), and these have prognostic implications.. For instance, diffuse erythema occurs in late stage disease in humans, and is a frequent (86%) and early finding in dogs. Also, we frequently see presence of tumour forms at onset in dogs, often in combination with other lesions, and this does not seem to affect prognosis. defined as &gt;1000 cells/mm3 in blood (or presence of T cell clone in blood) PR in humans usually distal extremities, vs dogs with foot pad involvement, often have other areas of body affected.
- The key histopathological diagnostic feature of epitheliotropic T-cell lymphoma is the tropism of the neoplastic lymphoid T cells for the epidermal or mucosal epithelium and the adnexal structures of the skin, in particular the wall of the hair follicles. The intraepithelial neoplastic lymphocytes are either diffusely distributed within the epithelium or form discrete aggregates (nests) referred to as “Pautrier’s microaggregates”, “Pautrier’s microabscesses” or “Pautrier collections”. Diffuse infiltrates of neoplastic T cells tend to remain in the lower levels of the epidermis. Tropism to the cutaneous adnexa may be more prominent than invasion into the epidermis, and complete obliteration of the hair follicles and adnexal glands of the skin may occur. Infiltration of apocrine sweat glands may be striking in some cases, and is highly diagnostic for epitheliotropic T-cell lymphoma since inflammatory infiltrates generally do not occur in such location. In addition, we know that the immunophenotypic features of epitheliotropic lymphomas of the skin of dogs are in most cases CD8+ Gaining information about whether CD8+ typical of canine ETL is only achievable with fresh snap-frozen tissue samples.
- due to the potential overlap- ie reactive T cell infiltrate in inflammatory disease/or equivocal results a.PCR looks for a typical T cell receptor (gamma) rearrangement, that tends to be conserved in this disease
- Response rates to CHOP, MOPP etc is around 86% OR (29% CR, 57% PR with small numbers treated, n=7)- duration short around 100 days in these dogs, usually considered to be around 3-5 mo. Pre reports of combo chemo showed responses of 2-16 weeks (14-112 d) Bexarotene (novel retinoid) Vorinostat Denileukin difitox
- Prednisolone, vincristine, cyclophosphamide, L-asparaginase, and recombinant-human interferon α-2a had been a.administered before this photograph was taken.
- Minicells were incubated with chemotherapeutic drugs and loading was evident with all drugs by red autofluorescence of Dox, or green fluoresnence of Vinblastine or Pac. Targeting of minicells was achieved by using biclonal Atb in which one arm recognizes the O antigen component of minicell surface LPS and other a cell surface receptor specific for the mamalian cell to be targeted. Drug packaging was dependent on to both drug concentration and time of incubation. Efflux has not been observed even with extensive minicell washing and incubation in drug-free solution.