1. Data
Changes in antimicrobial use and resistance rates pre- and five year
post-implementation of an antibacterial stewardship program
Spencer Donovan, PharmDc1, Haley Morrill, PharmD1,2, Kerry LaPlante, PharmD1,2,3
1The University of Rhode Island, College of Pharmacy, 2Providence Veterans Affairs Medical Center,
3Alpert Medical School of Brown University
Introduction
Purpose
Methodology
Conclusion
References
Antimicrobial stewardship programs have the potential to
reduce antibiotic use and slow the development of
resistance in various pathogens. This can be beneficial to
both patients and institutions by avoiding costly treatment
complications such as Clostridium difficile infection and
extended hospital stays. The purpose of this study was to
evaluate the changes in antibiotic use and pathogen
resistance rates following the implementation of an
antibacterial stewardship program.
An antimicrobial stewardship program (ASP) which utilized
prospective audit and feedback was formally implemented
at the VA Medical Center in Providence, RI in September
2012. The Providence VA Medical Center is a small
teaching hospital licensed for 119 beds. Using the CDC’s
National Healthcare Safety Network (NHSN) Antimicrobial
Use and Resistance options, antibiotic use using days of
therapy per 1000 patient days pre- and post-
implementation of this program were retrospectively
analyzed. Resistance rates in pathogens were also
evaluated.
Post-implementation of the ASP, resistance rates of many
pathogens remained stable to resistance rates pre-
implementation. Total antibiotic use decreased for most
antibiotics post-implementation of the ASP in recent years.
Antimicrobial stewardship programs are important for
reducing antibiotic use and limiting the propagation of
antimicrobial resistance.
1Moody J, Cosgrove S, Olmsted R, Septimus E, Aureden K, Oriola S, et al. Antimicrobial stewardship: A collaborative partnership between infection preventionists and health care epidemiologists. Am J Infect Control 2012;40:94-95
2Centers for Disease Control and Prevention. (2016). Core elements of hospital antibiotic stewardship programs. Retrieved from: http://www.cdc.gov/getsmart/healthcare/implementation/core-elements.html#_ENREF_12
Antimicrobial resistance rates have been increasing over
recent years, largely in part due to inappropriate
antimicrobial prescribing practices. Failure to deescalate
empiric therapy, drug-pathogen coverage mismatches, and
inadequate durations of therapy have all contributed to
rising antimicrobial resistance.1 In order to slow the rise of
resistance rates, many institutions have adopted
antimicrobial stewardship programs for the purposes of
monitoring antimicrobial resistance and implementing
protocols to decrease unnecessary antibiotic prescribing.2
Although these programs may reduce excess antibiotic
use overall, their effects on antimicrobial resistance rates
are less evident.
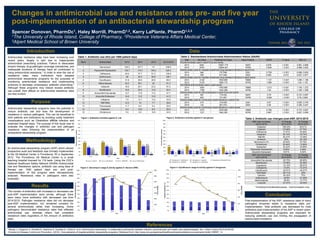
ABX Use Increased
(2012-2015)
% Change
2012-2015
% Change
2014-2015
Cefepime 166.04% 49.51%
Cefazolin 110.98% 47.74%
Ceftriaxone 77.57% 76.26%
Imipenem 55.14% -33.74%
Nafcillin 52.47% -12.48%
Amikacin 50% -93.18%
Vancomycin (IV) 30.93% 72.75%
Clindamycin 25.46% -13.69%
Aztreonam 22.42% -25.69%
Piperacillin/Tazobactam 8.92% 4.56%
Ampicillin/Sulbactam 6.61% 8.34%
ABX Use Decreased
(2012-2015)
% Change
2012-2015
% Change
2014-2015
Amoxicillin/Clavulanate -83.75% -80.95%
Moxifloxacin -75.96% -52.08%
Cephalexin -74.14% -69.07%
Cefotaxime -72.9% -72.37%
Ciprofloxacin -62.91% -40.27%
TMP/SMX* -60.71% -25%
Cefoxitin -54.35% 75%
Azithromycin -39.8% -21.28%
Metronidazole -36.8% -13.77%
Linezolid -27.27% -39.39%
Table 1. Antibiotic use (AU) per 1000 patient days
Rank Antimicrobial 2013 2014 2015 2013-2015
1 Vancomycin 120.3 107.7 111 338.9
2 Piperacillin/Tazobactam 105.7 110.3 104.2 320.2
3 Ceftriaxone 40.9 37.7 51.2 129.8
4 Azithromycin 48 40.3 39.8 128.1
5 Ciprofloxacin 31.8 26.9 26.8 85.5
6 Metronidazole 30.2 26.1 25 81.3
7 Cefazolin 18.9 25.1 23.2 67.2
8 Moxifloxacin 18.8 20.4 13.2 52.4
9 Amoxicillin/Clavulanate 12.7 17.8 17.2 47.7
10 Ampicillin/Sulbactam 14.9 13.2 13.5 41.5
11 Cefepime 7.5 13.1 13.2 33.9
12 TMP/SMX 12.3 10 7.7 29.9
13 Fluconazole 11.7 8.4 5.4 25.5
14 Imipenem 6.4 10.6 8.5 25.5
15 Clindamycin 5.5 8.2 10.8 24.5
*Trimethoprim/Sulfamethoxazole - Oral formulation only
Year AU Days Predicted AU Days Days Present SAAR P value 95% CI
All antimicrobials used in adult ICUs and wards
2014 9361 10657.775 18257 0.878 < 0.001 0.861, 0.896
2015 9793 10806.061 18785 0.906 < 0.001 0.888, 0.924
Antimicrobials used for hospital-onset/multi-drug resistant infections in adult ICUs
2014 560 737.648 2391 0.759 < 0.001 0.698, 0.824
2015 556 617.946 2003 0.900 0.012 0.827, 0.977
Antimicrobials used for hospital-onset/multi-drug resistant infections in adult wards
2014 2108 1853.689 15866 1.137 < 0.001 1.089, 1.186
2015 2129 1960.710 16782 1.086 < 0.001 1.04, 1.133
Anti-MRSA antimicrobials used in adult wards
2014 1654 1363.669 15866 1.213 < 0.001 1.155, 1.272
2015 1789 1442.399 16782 1.24 < 0.001 1.184, 1.299
Antimicrobials used for SSI prophylaxis in adult ICUs and wards
2014 567 718.024 18257 0.79 < 0.001 0.727, 0.857
2015 603 731.807 18785 0.824 < 0.001 0.76, 0.892
Antimicrobials used for community-onset infections in adult ICUs
2014 214 319.408 2391 0.67 < 0.001 0.585, 0.764
2015 123 267.575 2003 0.46 < 0.001 0.384, 0.547
Antimicrobials used for community-onset infections in adult wards
2014 1475 1876.068 15866 0.786 < 0.001 0.747, 0.827
2015 1721 1984.383 16782 0.867 < 0.001 0.827, 0.909
36% 37%
45%
42%
22%
25% 24% 25%
17%
21%
27% 28%
2% 3% 3% 3%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2012 2013 2014 2015
Percentantibioticresistant
Year
Figure 1. Antibiotics activities against E. coli
E.coli vs. Amp/sul E.coli vs. Ciprofloxacin E.coli vs. TMP/SMX E. coli vs. Nitrofurantoin
23% 24% 23% 22%
10%
12%
7%
5%
2%
5%
8%
6%
12%
10% 11%
7%
10% 10%
14%
11%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2012 2013 2014 2015
Percentantibioticresistant
Year
Figure 2. Antibiotics activities against P. aeruginosa
P. aeruginosa vs. Ciprofloxacin P. aeruginosa vs. Imipenem P. aeruginosa vs.Piperacillin/Tazo
P. aeruginosa vs. Cefepime P. aeruginosa vs. Ceftazidime
22% 24% 22% 20% 23% 24% 23% 22%
774
1028
904
827
604
492
375
224
0
200
400
600
800
1000
1200
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2008 2009 2010 2011 2012 2013 2014 2015
TOTALGRAMS
PERCENTRESISTANT(%)
Year
Figure 4. Ciprofloxacin usage & activity against P. aeruginosa
67%
80% 82% 81%
62% 62%
78%
25%
2081
4898
5796
6030
4920
4320
3729
6666
0
1000
2000
3000
4000
5000
6000
7000
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2008 2009 2010 2011 2012 2013 2014 2015
TOTALGRAMS
PERCENTRESISTANT(%)
Year
Figure 3. Vancomycin usage & activity against E. faecium (VRE)
The number of antibiotics with increased or decreased use
post-ASP implementation were similar, although there
were many more antibiotics with decreased use from
2014-2015. Pathogen resistance rates did not decrease
post-ASP implementation, but remained constant for
several antimicrobials rather than increasing. Some
pathogens demonstrated resistance rates that reflected
antimicrobial use, whereas others had consistent
resistance rates regardless of the amount of antibiotics
used.
Results
Table 3. Antibiotic use changes post-ASP, 2014-2015
Table 2. Standardized Antimicrobial Administration Ratios (SAAR)