Guillain barré syndrome
•
27 likes•7,191 views

Guillain-Barré syndrome is a rare autoimmune disorder where the immune system attacks the peripheral nervous system, causing muscle weakness and paralysis. It is considered a post-infectious disorder, often triggered by bacterial or viral infections. Clinically, it begins with pain, paresthesia, and weakness in the legs that ascends to the trunk and arms. Diagnosis involves lumbar puncture showing elevated proteins with normal cell counts and electrodiagnostic testing showing demyelination. Treatment focuses on supportive care like ventilation and immunotherapy using plasma exchange or IVIG. Recovery can take many months but most experience significant improvement.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Guillain barré syndrome
Similar to Guillain barré syndrome (20)
More from Tarika Sharma, Lecturer, CON, ILBS, New Delhi
More from Tarika Sharma, Lecturer, CON, ILBS, New Delhi (11)
Recently uploaded
Recently uploaded (20)
Guillain barré syndrome
- 1. GUILLAIN-BARRÉ SYNDROME Ms Tarika Sharma Assistant Professor MMCON, MMU, Ambala
- 2. Introduction Guillain-Barre syndrome is a rare but serious autoimmune disorder in which the immune system attacks healthy nerve cells of the peripheral nervous system.
- 3. Introduction… GBS is an acute inflammatory demyelinating polyneuropathy that is the most common cause of acute or subacute generalized paralysis. GBS is considered to be a postinfectious immune-mediated disease targeting peripheral nerves.
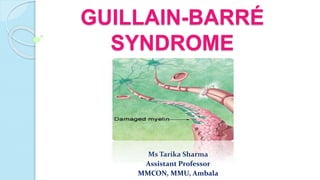
- 4. Definition Guillain-Barre syndrome (GBS) is an acute autoimmune disease marked by inflammation of the peripheral nerves, affecting arms and legs and Involves destruction of the myelin sheath surrounding largest, most myelinated sensory and motor fibers, resulting in disrupted proprioception and weakness.
- 8. Epidemiology 1-2 (1.9) per 100,000 persons . most commonly it affects young and middle- aged adults 30 to 50 years of age. Females slightly more affected than males. More common in devloping countries. Germany (7.9%), Mexico (44%), India (28%).
- 9. Etiology The precise cause of Guillain-Barre is unknown. Sixty percent of cases have followed a lung infection or a gastrointestinal infection . The following infections have been associated with Guillain-Barre: Campylobacter jejuni infection. Influenza (the flu) Cytomegalovirus (a strain of the herpes virus) Epstein-Barr virus infection (mononucleosis) Mycoplasma pneumonia HIV
- 10. Triggers of GBS Surgery Trauma Pregnancy Hodgkin’s disease HIV
- 11. PathophysiologyInfectious organism contains an amino acid – mimics peripheral nerve myelin protein. Cell mediated immune attack on peripheral nerve myelin protein Immune system cannot distinguish between the 2 proteins Attack and destroys peripheral nerve myelin Inflammation and destruction of myelin sheath Axon is unable to support
- 12. Pathophysiology… Specific immune response directed against PNS antigen is initiated Auto antigen T cells circulate & enter the PNS Auto antigen is recognised by T cells Activation of local macrophages& B cells to secrete auto antibodies
- 13. Cont.. Blood nerve barrier breaks down, leading to entrance of specific auto antibodies into nerve which cross react with myelin Multifocal stripping of myelin Defects in propagation of electrical nerve impulses Conduction block &flaccid paralysis
- 15. Disease Progression 80% experience complete recovery Recovery may last from 2 months to 2 years 3 distinct phases: Acute (4 wks) - initial rapid onset of symptoms Plateu (few days to few weeks) - symptoms neither worsen nor improve Recovery - gradual improvement
- 16. Clinical Features Initially Pain in the muscle Weakness of muscle The onset is gradual and progresses over days or weeks. By the 3rd week 90% of the patient are weak. Usually begins in the lower extremities and progressively involves the trunk, the upper limbs, and finally the bulbar muscles. This pattern is known as Landry ascending paralysis. Relatively symmetrically, but asymmetry is found in 9% of patients Paresthesias occur in some cases.
- 17. Clinical Features… Respiratory insufficiency due to Intercostal and diaphragmatic muscle paralysis Dysphagia and facial weakness Papilledema oculomotor and other cranial neuropathies The autonomic nervous system involvement: lability of blood pressure and cardiac rate, postural hypotension, episodes of profound bradycardia occasional asystole
- 18. Diagnosis Physical Assessment, Vital signs (tachycardias, bradycardias, Tachypnea, Blood pressure lability, bladder retention, paralytic ileus) Cranial nerves: Facial weakness, facial droop, dysphagia, dysarthria,Ptosis from cranial nerve III (oculomotor) palsy often is associated with limited eye movements. Reflexes are absent or hyporeflexic, Pathologic reflexes, such as Babinski, are absent.Hypotonia can be observed with significant weakness
- 19. Lab Studies CSF studies: During the acute phase of GBS ,an elevation in CSF protein (>0.55 g/L) without an elevation of white blood cells (<10 lymphocytes/mL). Complete blood counts Serologic studies ( increase in titre for infectious agent)
- 20. Diagnosis… Electromyography (EMG) studies Abnormalities in the NCS consistent with demyelination are sensitive and represent specific findings for classic GBS. MRI Pulmonary function tests Histologic Findings: Lymphocyte and macrophage infiltration is observed on microscopic examination of peripheral nerves.
- 22. Management… Mechanical ventilation Trachesotomy Sustained hypertension (ACE inhibitors, Beta blockers) Postural hypotension Urinary difficulties Ventilator support Autonomic dysfunction
- 23. Naso gastric tube Hyperalimentation Plasma exchange Intravenous immunoglobulin Nutritional support Immune therapy Management…
- 25. POTENTIAL COMPLICATIONS Breathing difficulties Heart and blood pressure problems Residual numbness or other sensations Pain Bowel and bladder function problems Blood clots Pressure sores
- 26. Nursing management Nursing Assessment Assess pain level due to muscle spasms and dysthesias. Assess cardiac function including orthostatic Blood Pressure. Assess respiratory status closely to determine hypoventilation due to weakness. Perform cranial nerve assessment, especially ninth cranial nerve for gag reflex. Assess motor strength.
- 27. Nursing Diagnosis Ineffective Breathing Pattern related to weakness/paralysis of respiratory muscles Impaired Physical Mobility related to paralysis Imbalanced Nutrition: Less Than Body Requirements, related to cranial nerve dysfunction
- 28. Cont….. Impaired Verbal Communication related to intubation, cranial nerve dysfunction Chronic Pain related to disease pathology Anxiety related to communication difficulties and deteriorating physical condition
- 29. Patient education Advise patient and family that acute phase lasts 1 to 4 weeks, then patient stabilizes and rehabilitation can begin; however, convalescence may be lengthy, from 3 months to 2 years. Instruct patient in breathing exercises or use of incentive spirometer to reestablish normal patterns. Teach patient to wear good supportive and protective shoes while out of bed to prevent injuries due to weakness and paresthesia.
- 30. Cont…. Instruct patient to check feet routinely for injuries because trauma may go unnoticed due to sensory changes. Reinforce maintenance of normal weight; additional weight will further stress the motor abilities. Encourage the use of scheduled rest periods to avoid over-fatigue.
- 31. Thank you….
Editor's Notes
- Proprioception: the series of events by which an org. senses the position , location, orientation, movement of the body and its parts.