5. Clinical manifestations
Stones in the renal pelvis may be associated with an
intense ,deep ache in the costovertebral region.
Hematuria
Pyuria
Pain originating in the renal area radiates anteriorly and
downward the bladder in the female and toward the
testis in male
Tenderness
Nausea and vomiting appear
These GI symptoms are due to renointestinal reflexes
and the anatomic proximity of the kidneys to the
stomach, pancreas ,and large intestine
6.
7. Assessment and diagnostic
By x-ray of the kidneys .
ureters And bladder(KUB)
Ultrasonography
Iv urography
Retrograde pyelography
24-hour urine test
11. Nutritional therapy
Increase fluid intake is the mainstay
a-calcium stones. Patient with calcium-based renal
stones were advised to restrict calcium in their diet.
B-uric acid stones .low-purine diet .foods high in
purine
(shellfish,anchovies,asparagus,mushroom,and
organ meats)
C-cystine stones .a low-protein diet
D-oxalate stones .
Intake of oxalate is limited
Theses include spinach
strawbrries,rhubarb,chocolate,tea,peanuts ,and
wheat barn.
12. Patien education
Preventing kidney stones
Avoid protein intake
Low-calcium diets
Avoid intake of oxalate-containing food
(eg.spinach,strawberries ,rhubarb ,tea
,peanuts ,wheat bran)
Increase drink fluid
Drink two glasses of water at bedtime
Avoid dehydration.
Avoid urinary tract infection
13. Interventional procedures
Ureteroscopy. extracorporeal shock wave
lithotripsy(ESWL)
(percuta-neous)stone removal
1. Ureteroscopy involves first visualizing the stone
and then destroying it .access to the stone is
accomplished by inserting a ureteoscope into the
ureter and then inserting a laser .electrohydraulic
lithotriptor,or ultrasound device through the
ureleroscope to fragment and remove the stones
2. ESWL is a noninvasive procedure used to break
up stones in the calyx of the kidney
14.
15.
16. Nursing care of…………….
Fragmented to the size of grains of sand , the
remnants the stones are spontaneously voided.
ESWL shock wave
Discomfort from the multiple shocks may occur .
. The patient is observed for obstruction and
infection result mg form blockage of the urinary
tract by stone fragments
.I urine is strained after the procedure
. voided gravel or and is sent to the laboratory
.Early ambulate
. Endourologic methods of stone removal maybe
used to extract renal
calculi the cannot be removed by other procedures
17. Surgical management ;
is indicated if the stone does not
respond to other forms of treat
ment nephrolithotomy (incision
incision into the kidney with
removal of the stone ) or a
nephrectomy, if the kidney is
nonfunctional secondary to
infection or hydronephrosis.
Stones in the kidney pelvis are
removed by a pyelolithotomy and
those in the bladder by cystotomy
18. Diagnosis
Nursing Diagnosis
1. Acute pain related to
inflammation obstruction
and abrasion of the urinary
tract
2 . Deficient knowledge
regarding prevention of
recurrence of renal stones
20. Manitoring and managing
Potential Complications
1. Increased fluid intake to prevent dehydration and
increase hydrostatic pressure .
2. The total urine output and patterns of voiding are
monitored .
3. Ambulation is encouraged
4. All urine is strained through gauze because
5. patient is instructed to report decreased urine
volume and bloody or cloudy urine
6. frequent nursing observation to detect the
spontaneous passage of a stone
7. Vital signs, including temperature, are monitored
21. Prgmoting Hama and community-based
care
Including maintaining a high fluid intake
Diet: decreas calcium in the food
avoiding habit: avoid stay under the sun
for along time
Exersic : walking at least 3ment/day
22. Follow up: first vist after one
week second vist after one
month thierd vist after three
month in one year after six
month in tow year than once
yrealy increase fluid intake
3L/day
23. Urine cultures may be performed
every 1 to 2 months the first
year and periodically thereafter
Recurrent UTI is treated
vigorously
24. Urine cultures may be
performed every 1 to 2
months the first year and
periodically thereafter
Recurrent UTI is treated
vigorously
25. If ESWL
1 increase fluid intake to assist in the
passage of stone fragments.
2 Family are instructed about signs and
symptoms that indicate complication
3 Inform the patient to expect hematuria
4 temperature
5 pain is unrelieved by the prescribed
medication
--------------------
Assess the patient understanding of
ESWL
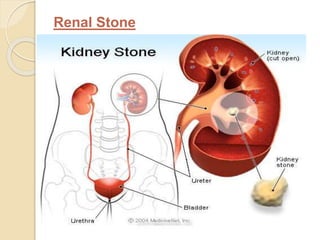
تحص بولي وتحصي الكلية تشير إلى الحجارة (الحصوات) في المسالك البولية والكلى
وتظهر مواقع مختلفة تشكيل الحصوات في المسالك البولية OC في الشكل.
قد تترافق الحجارة في الحوض الكلوي مع، آلام عميقة مكثفة في المنطقة الضلعي الفقري. بيلة دموية بيلة قيحية منشؤها ألم في منطقة الكلى يشع الأمامية وهبوط المثانة في الأنثى والخصية في نحو الذكور حنان الغثيان والقيء تظهر هي هذه الأعراض المعدية المعوية بسبب كلوي معوي ردود الفعل والقرب التشريحية للكلى إلى المعدة والبنكرياس، والأمعاء الغليظة
بواسطة الأشعة السينية للكلى. الحالب والمثانة (KUB) الموجات فوق الصوتية رابعا تصوير الجهاز البولي تصوير الحويضة بالطريق الراجع اختبار البول على مدار 24 ساعة
مسكنات الأفيونية غير الستيرويدية المضادة للالتهابات المخدرات (المسكنات)
زيادة السوائل في الجسم هو الدعامة الحجارة الكالسيوم. ونصح المريض مع القائم على الكالسيوم حصيات كلوية لتقييد الكالسيوم في نظامهم الغذائي. -B حصوات حمض اليوريك. نظام غذائي منخفض البيورين. الأطعمة التي تحتوي على البيورين (المحار، والأنشوجة، والهليون، الفطر، والجهاز اللحوم) الحجارة C-سيستين. اتباع نظام غذائي منخفض البروتين الحجارة D-أكسالات. تناول أكسالات محدودة وتشمل الأطروحات الفراولة والسبانخ، والراوند، والشوكولاته، والشاي، والفول السوداني، والقمح الحظيرة.
منع حصوات الكلى تجنب تناول البروتين الوجبات الغذائية منخفضة الكالسيوم تجنب تناول الأغذية التي تحتوي على الأكسالات (eg.spinach والفراولة والراوند، والشاي، والفول السوداني، ونخالة القمح) زيادة السوائل الشراب شرب كأسين من الماء قبل النوم تجنب الجفاف. تجنب التهاب المسالك البولية