Presentation1.pptx, radiological imaging of inner ear diseases
•Download as PPTX, PDF•
75 likes•11,136 views

This document discusses radiological imaging of inner ear diseases. It begins with cross sectional anatomy of the inner ear on CT and MRI. It then provides a classification of congenital malformations of the inner ear, including those limited to the membranous labyrinth and those involving both the osseous and membranous labyrinth. Examples of specific malformations are discussed such as Michel deformity, common cavity, cochlear aplasia, hypoplasia, incomplete partition, and semicircular canal anomalies. The document also discusses inflammatory lesions of the inner ear, facial nerve lesions including Bell's palsy and facial nerve schwannomas, and other pathologies such as aberrant arteries and dehis

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Presentation1.pptx, radiological imaging of inner ear diseases
Similar to Presentation1.pptx, radiological imaging of inner ear diseases (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Presentation1.pptx, radiological imaging of inner ear diseases
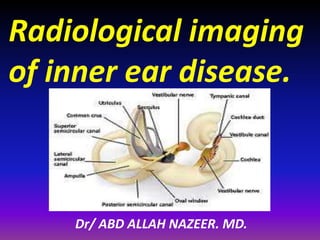
- 1. Radiological imaging of inner ear disease. Dr/ ABD ALLAH NAZEER. MD.
- 14. Cross CT sectional anatomy of the inner ear.
- 15. Cross MR sectional anatomy of the inner ear..
- 16. Cross MR sectional anatomy of the inner ear..
- 19. A classification of congenital malformations of the inner ear I. Malformations limited to the membranous labyrinth A. Complete membranous labyrinthine dysplasia (Siebenmann-Bing) B. Limited membranous labyrinthine dysplasia 1. Cochleosaccular dysplasia (Scheibe) 2. Cochlear basal turn dysplasia (Alexander) II. Malformations of the osseous and membranous labyrinth A. Complete labyrinthine aplasia (Michel) B. Cochlear anomalies 1. Cochlear aplasia 2. Cochlear hypoplasia 3. Incomplete partition (Mondini) 4. Common cavity C. Labyrinthine anomalies 1. Semicircular canal dysplasia 2. Semicircular canal aplasia D. Aqueductal anomalies 1. Enlargement of the vestibular aqueduct 2. Enlargement of the cochlear aqueduct E. Internal auditory canal abnormalities 1. Narrow internal auditory canal 2. Wide internal auditory canal.
- 21. Michel deformity 6% Cochlear aplasia 5% Common cavity 8% Cochlear hypoplasia 12% Incomplete Partition 41% IP-I (Cystic cochleovestibular malformation) 20% IP-II (Mondini deformity) 19% IP-III (X-linked Deafness) 2% LVAS 15%
- 22. Complete labyrinthine aplasia (Michel) The severest deformity of the membranous and osseous labyrinth, complete labyrinthine aplasia, was first described by Michel (1863). This malformation is exceedingly rare. Presumably, a developmental arrest occurs before the formation of an otic vesicle, resulting in a complete absence of inner ear structures. Complete labyrinthine aplasia has been reported in association with anencephaly and thalidomide exposure . A recent purported case of Michel's dysplasia actually described a cystic inner ear of the common cavity type. The incidence of complete labyrinthine aplasia is overestimated in the radiographic literature because it is confused with labyrinthine ossification. In the latter condition, which is usually acquired during life, a sizable and dense otic capsule is present radiographically. In complete labyrinthine aplasia, the otic capsule is entirely absent. Such ears are of course uniformly deaf. HRCT: Show complete absence of inner ear with hypoplasia of the petrous bone and narrow atretic ISC. Absence of round and oval window. Flattening of medial wall of middle ea cavity. MRI: 8th cranial nerve not visualized on MR images associated wih skull base, CVJ vascular anomalies.
- 23. Michel aplasia. The labyrinth is absent on the right (black arrow), whereas the left cochlea is normal on computed tomography (white arrow). The right internal auditory canal is narrow and contains only the facial nerve (thin white arrow). The volume of the right petrous temporal bone is smaller than that of the left.
- 26. Common cavity A deformed inner ear in which the cochlea and vestibule are confluent, forming an ovoid cystic space without internal architecture, may be explained by an arrest at the fourth week otocyst stage. Alternatively, it may result from aberrant development at a later stage. An empty ovoid space typically longer in its horizontal dimension is seen adiographically. Although the size of the cyst may vary, it averages 7 mm vertically and 10 mm horizontally. It is quite easy to misdiagnose a dysplastic lateral SCC as a common cavity deformity. The key to differentiating between them is that a common cavity cochlea lies predominantly anterior to the internal auditory canal (IAC) on axial plane CT, and a dysplastic vestibular system lies posterior to it. Histologically, an ovoid or spherical smooth-walled cystic cavity containing a primordia of the membranous labyrinth has been described. Sensory and supporting cells may be differentiated into recognizable organs of Corti that are scattered peripherally around the walls of the cyst. Neural population is usually sparse or absent. Hearing is usually, but not invariably, poor.
- 29. Common cavity deformity on computed tomography (CT) (A) and fast imaging employing steady-state acquisition (FIESTA) magnetic resonance imaging (MRI) (B). A septation (thin white arrow—B) seen on FIESTA divides the primitive cochlea anteriorly (white arrow—A,B) from the fused vestibule and semicircular canals posteriorly (black asterisk). Note that a portion of the posterior semicircular canal has formed (black arrows). Note the anomalous course of the common cochleovestibular nerve (white arrowheads) in the internal auditory canal. Note the labyrinthine segment of the fallopian canal on CT (black arrowhead—A) and the facial nerve in the internal auditory canal (black arrowhead—B).
- 30. Cochlear aplasia In this deformity the cochlea is completely absent, presumably as a result of an arrest in the development of the cochlear bud at the fifth week. This morphologic pattern is rare. Radiographically, only a vestibule and SCCs (usually deformed) are present. To differentiate this anomaly from labyrinthine ossification it is necessary to assess the amount of otic capsule bone anterior to the internal auditory canal. In cochlear aplasia, the otic capsule is absent, whereas in osseous obliteration it is dense and of normal dimensions. Ears with cochlear aplasia are devoid of auditory function. Imaging features: 1- Absence of cochlea. 2- Dilatation of the vestibule. 3- Deformity of semicircular canal. 4- Dense otic bone.
- 31. Atresia of the cochlear foramen to the left and normal cochlear foramen to the right and non-visualization of the left cochlear nerve.
- 33. Cochlear hypoplasia. An arrest during the sixth week results in a hypoplastic cochlea consisting of a single turn or less. This deformity comprises approximately 15% of all cochlear anomalies. Radiographically, a small bud of variable length (usually 1 to 3 mm) protrudes from the vestibule as compared to normal height of 12-13 mm. Abnormal small IAC. The vestibule is frequently enlarged with accompanying semicircular malformations in about half of faces. Small cochlear lacking a modiolus or other internal architecture have been described histologically . Hearing is variable in these ears and may be remarkably good considering the minute size of the cochlea. The variability of hearing presumably is accounted for by degree of membranous labyrinthine development within the truncated cochlear lumen.
- 35. Incomplete partition (Mondini) Arrest at the seventh week stage yields a cochlea that has only 1.5 turns. This is the most common type of cochlear malformation, accounting for over 50% of all cochlear deformities. Radiographically, the cochlea is smaller than normal and partially or completely lacks an interscalar septum . Although the usual cochlea measures 8 to 10 mm vertically, it is typically in the 5 to 6 mm range with incomplete partition deformity. Care must be exercised in counting the number of cochlear turns radiographically, as this may be difficult to determine even on high- resolution CT scans. The radiographic diagnosis depends more on cochlear size and the absence of a scalar septum than on the number of cochlear 8 turns perceived. Histologically, incomplete partition appears to be the radiographic correlate of classical Mondini's dysplasia. In numerous reported cases a small cochlea with 1.5 turns possessing an apical scala communis due to deficiency in the osseous spiral lamina has been described. Organ of Corti development is variable as is auditory neural population. As might be expected, auditory function is also variable, ranging from normal to profound deafness. The mean hearing threshold (three tone average) in a group of 41 incomplete partition ears was 75 dB.
- 37. Classic Mondini malformation (incomplete partition type II.
- 40. Semicircular canal dysplasia Dysplasia of the lateral SCC is a common type of inner ear malformation. Approximately 40% of ears with a malformed cochlea will have an accompanying dysplasia of the lateral SCC. Occasionally, dysplasia of the lateral SCC exists as the sole inner ear malformation. The lateral SCC is deformed more often than the posterior or superior SCC, apparently because it forms earlier in embryogenesis. The typical radiographic appearance of SCC dysplasia is that of a short, broad cystic space confluent with the vestibule. Semicircular canal aplasia SCC aplasia is only one-fourth as common as SCC dysplasia. It is usually associated with cochlear anomalies. Presumably, it arises from a failure in the development of the vestibular anlage before the sixth week.
- 41. Axial CT image reveals fusion of the vestibule and LSC, forming a cystic lumen on the left side (curved arrow). On the contralateral side, there is both a narrow internal auditory canal and dysplastic vestibule-rudimentary LSC.
- 42. Vestibular dysplasia with LEDS.
- 45. Bilateral vestibular aqueduct syndrome.
- 46. Enlarged vestibular aqueduct with modiolar dysplasia (Mondini malformation). Fast imaging employing steady-state acquisition (FIESTA) magnetic resonance image (MRI) of right inner ear (A) shows enlarged endolymphatic sac expanding the vestibular aqueduct (thick white arrow) as compared with the normal posterior SCC (arrowheads). The osseous spiral lamina and modiolus (thin white arrow) are hypoplastic. Compare with the normal FIESTA MRI of the left inner ear (B). Note that the vestibular aqueduct is typically only faintly visualized on FIESTA (thick black arrow) and normal cochlea and modiolus (thin black arrow).
- 47. Developmental Anomalies of the Internal Auditory Canal Narrow internal auditory canal: A narrow IAC may indicate a failure of eighth nerve development. When a patient has normal facial function and an IAC less than 3 mm in diameter, it is likely that the bony canal transmits only the facial nerve. A narrow IAC may accompany inner ear malformations or may be the sole radiographically detectable anomaly in a deaf child. A narrow IAC has been considered a relative contraindication to cochlear implantation. Wide internal auditory canal: Unlike congenital narrowness of the IAC, a congenitally large canal may be an incidental finding in normal individuals. When a large IAC (> 10 mm in diameter) accompanies a malformation of the inner ear, it does not, as an independent variable, correlate with the level of hearing. The importance of detecting enlargement of the IAC is its association with spontaneous CSF leak and gusher during stapes surgery .
- 48. Narrow Internal Auditory Canal with Duplication in a Patient with Congenital Sensorineural Hearing Loss
- 49. Narrowing of the left internal auditory canal with absence of left cochlear nerve.
- 53. Labyrinthitis. T1-weighted magnetic resonance image (T1W MRI) with (B) and without (A) contrast shows dramatic enhancement of the cochlea (black arrows) and vestibule (white arrows), indicating labyrinthitis.
- 54. Intralabyrinthine hemorrhage in a patient with endolymphatic sac tumor (not shown). Hyperintense signal on noncontrast T1-weighted magnetic resonance image (T1W MRI) fills the vestibule and a portion of the posterior SCC (white arrow—A). On fast-spin echo T2-weighted magnetic resonance image (T2W MRI) (white arrow—B) the vestibule is poorly visualized because of signal loss from blood. Note the normal appearance of the cochlea on both the noncontrast T1W and T2W MRI (white arrowheads—A,B).
- 56. Ossified bony left labyrinth and cochlea
- 57. Labyrinthitis ossificans of the left superior semicircular canal
- 62. Petrous apex cholesterol granuloma.
- 64. Petrous apicitis. MRI show fluid signal on T1-wi and T2-wi in right and left air cells of PA & mastoid complex (arrows). Post-contrast T1-wi (with fat-sat) demonstrate CE (arrowheads) on the right mastoid and extension into right cavernous sinus, and skull base osteomyelitis (arrowheads), prevalent on the right side.
- 68. Aberrant internal carotid artery.
- 76. Criteria: Unilateral Peripheral Acute onset No apparent cause Does not involve any other cranial nerves. Pathogenesis: Secondary to swelling and edema of the 7th nerve within the fascial nerve canal.
- 78. Bell's palsy is a form of facial paralysis resulting from a dysfunction of the cranial nerve VII (the facial nerve) causing an inability to control facial muscles on the affected side. Several conditions can cause facial paralysis, e.g., brain tumor, stroke, myasthenia gravis, and Lyme disease. However, if no specific cause can be identified, the condition is known as Bell's palsy. Named after Scottish anatomist Charles Bell, who first described it, Bell's palsy is the most common acute mononeuropathy(disease involving only one nerve) and is the most common cause of acute facial nerve paralysis (>80%). Bell's palsy is defined as an idiopathic unilateral facial nerve paralysis, usually self-limiting. The hallmark of this condition is a rapid onset of partial or complete paralysis that often occurs overnight. In rare cases (<1%), it can occur bilaterally resulting in total facial paralysis. It is thought that an inflammatory condition leads to swelling of the facial nerve. MRI show enhancement of the fascial nerve within the tympanic portion of the fascial nerve canal which support the diagnosis.
- 80. Bell palsy
- 82. Bell palsy:
- 83. Facial nerve schwannoma A facial nerve schwannoma (FNS) (also known as facial nerve neuroma / neurilemoma) a schwannoma that arises from the facial nerve. They are generally uncommon, and when involving the temporal bone and make up less than 1% of all temporal bone tumours. Pathology As schwannomas elsewhere they originate from the surface of the nerve, and displace and splay the nerve fibers over their eccentric growth (this compares favorably to neurofibromas through which the axons are distributed). This allows for potential resection of the tumour while sparing the nerve. Similar to acoustic schwannomas, they may grow to a quite sizable extent and exert positive mass effect with growth into the cerebellopontine angle. Clinical presentation They can present with a wide variety of symptoms. More frequently they present with gradual, and often incomplete, facial nerve palsy. Rapid onset mimicking a Bell's palsy is certainly also recognised. Mass effect on adjacent nerves may well cause sensory neural hearing loss (SNHL) or even conductive hearing loss if growth into the middle ear impairs the normal function of the ossicles. In a minority of cases ( ~10%) the tumour is extra cranial, where it presents as an asymptomatic parotid mass.
- 84. Radiographic features Imaging characteristics of the tumour itself is the same as that of schwannomas elsewhere : homogenous enhancement on both CT and MRI when small; heterogenous when large. The best clue that a schwannoma is of the facial nerve rather than the more common vestibulochoclear nerve (CN VIII) is expansion extending along the facial nerve canal - especially along the labyrinthine segment. CT In all cases, hi resolution thin section bone CT of the temporal bone is required to assess the otic capsule. Bony scalloping and remodeling may be present. Failure to preoperatively diagnose bony erosion can lead to postoperative fistula formation. MRI Signal characteristics include T1 - typically iso- to hypo intense relative to gray matter T2 - typically hyperintense ; large lesion may show heterogenous signal T1 C+ (Gd) - usually demonstrate homogeneous enhancement with larger lesions with cystic degeneration seen as focal intramural low signal intensity.
- 86. Left Facial nerve schwannoma
- 87. Right geniculate ganglion facial nerve schwannoma.
- 88. Left tympanic segment facial nerve schwannoma.
- 89. Facial nerve hemangioma A facial nerve hemangioma is a benign vascular tumour of the facial nerve. This and facial nerve schwannomas make up the majority of primary tumours of the facial nerve, which are very rare entities(0.7%). Pathology Location: It has a predilection for the region around the geniculate ganglion (although even more rarely seen in the IAC), compared to schwannomas which can occur anywhere along the nerve. Radiographic features MRI T1 - iso or slightly hypo intense T2 - hyper intense C+ Gd - intense contrast enhancement Differential diagnosis Imaging differential considerations include facial nerve schwannoma facial nerve malignant schwannoma facial nerve perineurioma meningioma arising from the geniculate ganglion have been reported facial nerve metastases, hematogenous and retrograde spread.
- 91. Hemangioma. Ax/Cor CT images show a poorly marginated mass of geniculate fossa with typical amorphous “honeycomb” bone changes (arrows), post gadolinium T1-wi demonstrate avid CE with foci of low signal (arrows).
- 92. Ménière's disease also called endolymphatic hydrops, is a disorder of the inner ear that can affect hearing and balance to a varying degree. It is characterized by episodes of vertigo, low-pitched tinnitus, and hearing loss. The hearing loss is for some time fluctuating rather than permanent, meaning that it comes and goes, alternating between ears, then becomes permanent with no return to normal function. The condition affects people differently; it can range in intensity from being a mild annoyance to a lifelong condition. Clinical finding: 1- Fluctuating hearing loss. 2- Episodic vertigo. 3- Tinnitus. 4- Sensation of fullness in the ears.
- 93. Imaging The role of imaging is controversial2, but improved spatial resolution in CT and MRI is likely to show where endolymphatic flow is impaired. MRI MRI is used to exclude alternative diagnoses such as vestibular schwannoma or other cerebellopontine angle lesions, and superior canal dehiscence. High resolution MRI can show lack of a visible endolymphatic duct and sac. The gadolinium successfully penetrate the round window membrane, entering the perilymphatic space and delineating the contrast enhanced perilymphatic and contrast- negative endolymphatic spaces of the inner ear. CT Reduced visualization of saccular duct and endolymphatic sinus are features.6 At high-resolution temporal bone CT, the vestibular aqueduct is either small or not visible at all, in contrast to the congenital large vestibular aqueduct syndrome.
- 95. Grade 1 imaging findings in 61-year-old woman in nonacute phase of Meniere disease with high-frequency hearing loss. A–D, Affected left ear. E–H, Unaffected right ear. Bilateral endolymphatic sacs (arrows) are clearly visible.
- 96. Grade 2 imaging findings in 34-year-old woman in nonacute phase of Meniere disease with high-frequency hearing loss. There is poor visibility of the contents of the vestibular aqueduct in the affected left ear (A–D) as compared with the unaffected right ear (E–H). Arrows show the endolymphatic duct and sac. Note difference in visibility between the affected side and the unaffected side.
- 97. Grade 3 imaging findings in 28-year-old woman in nonacute phase of Meniere disease. In the affected right ear (A–E), the endolymphatic duct and sac are not delineated. However, the endolymphatic duct and sac (arrows) can be seen in the unaffected left ear (F–J).
- 98. Grade 3 imaging findings in 34-year-old woman in nonacute phase of Meniere disease with flat hearing impairment. The affected left ear (A–D) does not show the endolymphatic duct and sac; however, the endolymphatic duct and sac are clearly visible in the unaffected right ear (E–H).
- 99. Grade 3 imaging findings in a 21-year-old man in the acute phase of Meniere disease. In the affected right ear (A–D), the endolymphatic duct and sac are not delineated. However, the endolymphatic duct and sac (arrows) can be seen in the unaffected left ear (F–I).
- 100. Endolymphatic sac tumour Endolymphatic sac tumours (ELST) are very rare, locally invasive tumors of endolymphatic sac. Early detection of ELST is very important, because early surgical intervention may prevent further hearing loss. Presentation of tumour is: hearing loss : 95 %, acute in 43% and stepwise in second half tinnitus : 92% vertigo or disequilibrium : 62% aural fullness : 29% facial paresis : 8% Radiographic features CT When visible, it gives a picture of bone erosion and the "moth-eaten" petrous bone. ELSTs commonly enhance intensely on CT. MRI Signal characteristics include T1: may show high-density T1 C+ (Gd): typically show enhancement in the non-cystic component of the tumour. T2: often of heterogenous signal.
- 101. Endolymphatic sac tumor. T1-weighted (T1W) precontrast (A) and postcontrast (B) magnetic resonance image (MRI) show a hyperintense enhancing lesion (white arrow, B) in the right petrous bone at the expected position of the endolymphatic sac. Note hyperintensity (white arrows, A, D) on precontrast T1W (A) and T2-weighted (T2W) (D) MRI caused by hemorrhagic and proteinaceous elements of the tumor. Computed tomography demonstrates erosion of temporal bone (black arrow—C) adjacent to the vestibular aqueduct (black arrowheads—C), which is characteristic of this tumor.
- 102. MRI T1 weighted images of the brain, showing a very large ELST of the left temporal bone, in axial view on the left and coronal view on the right. There has been complete erosion of the petrous temporal bone by the tumor, with significant brainstem and cerebellar compression.
- 104. Tumour which has relation to the with inner ear.
- 105. Vestibular schwannoma Acoustic schwannoma is a relatively common type of tumour which arises from the vestibulochoclear nerve (CN VIII). Bilateral acoustic schwannomas are strongly suggestive of neurofibromatosis type 2 (NF2). Epidemiology. They account for 7-8% of all primary intracranial tumours and 75-90% of cerebellopontine angle masses . Bilateral vestibular schwannomas are highly suggestive of neurofibromatosis type 2 (NF2)), although bilateral tumours are encountered in the familial form of acoustic schwannomas in the absence of other stigmata of NF2. Origin: Most from inferior vestibular nerve, at glial-schwann cell interface. Clinical presentation. The typical presentation is with sensorineural hearing loss or tinnitus. In some patients this goes unnoticed and presentation is delayed until the lesion is much larger and presents with mass effect. Possibilities include cerebellar and brainstem symptoms (e.g. other cranial nerve dysfunction), or hydrocephalus due to effacement of the fourth ventricle.
- 106. Radiographic features: CT May show erosion and widening of the internal acoustic meatus. The density of these tumours on non-contrast imaging is variable, and often they are hard to see, especially on account of beam hardening and streak artefact form the adjacent petrous temporal bone. Contrast enhancement is present, but can be underwhelming, especially in larger lesions with cystic components. MRI T1 Slightly hypo-intense c.f. adjacent brain – 63% iso intense c.f adjacent brain – 37% may contain hypo intense cystic areas T2 Heterogeneously hyper intense c.f to adjacent brain cystic areas fluid intensity. may have associated peri-tumoural arachnoid cysts . T1 C+ (Gd) Contrast enhancement is vivid but heterogeneous in larger tumours
- 107. Intralabyrinthine schwannoma. T1-weighted postcontrast magnetic resonance image depicts an abnormally enhancing lesion within the left vestibule (white arrow). Note that the imaging findings may be indistinguishable from labyrinthitis.
- 109. VIII cn schwannoma. Illustration from Diagnostic Imaging, head and neck (Harnsberger et al.) When filling up the IAC schwannoma typically resembles an “ice cream cone”. Signal intensity is low on T1-wi, heterogeneous but predominant high on T2-wi. SSFP better demonstrate enlarging IAC mass. CE is marked and homogenous.
- 110. Bilateral vestibular schwannomas in a patient with neurofibromatosis 2 (NF2). (A, B) Axial and coronal T1 weighted images with gadolinium enhancement are shown. Note the presence of an associated trigeminal schwannoma (arrow). (C, D) Significant enlargement has occurred over four years, with the left sided vestibular schwannoma causing displacement of the brainstem.
- 111. IAC schwannoma and meningioma in patient with NF-2.
- 112. Meningiomas are a diverse set of tumors arising from the meninges , the membranous layers surrounding the central nervous system. They arise from the arachnoid "cap" cells of the arachnoid villi in the meninges. These tumors are usually benign in nature; however, a small percentage are malignant . 2nd most common CPA tumour(10%), usually arising from the meninges covering posterior petrous bone, More common in female than male(3-1). CT : 60% slightly hyperdense to normal brain, 20-30% have some calcification , 72% brightly and homogenously contrast enhance, less frequent in malignant or cystic variants. MRI : Signal characteristics include: T1 - isointense: 60-90%. somewhat hypointense: 10-40% compared to grey matter T1 C+ (Gd) - usually intense and homogenous enhancement T2 - isointense: 50%, hyperintense: 35-40% DWI - atypical and malignant sub types may show greater than expected restricted diffusion although recent work suggests that this is not useful in prospectively predicting histological grade.
- 115. Meningioma. T1-weighted postcontrast magnetic resonance image demonstrates a uniformly enhancing mass (black arrow) in the right cerebellopontine angle. Note the broad-based dural attachment on the petrous bone and small dural tails.
- 116. Epidermoid. Magnetic resonance image shows enlargement of the left cerebellopontine angle (CPA) (white arrows), with mass effect on the brainstem. Signal matches that of cerebrospinal fluid (CSF) on T1-weighted (A) and T2-weighted (B) images. Hyperintensity on diffusion-weighted imaging (C) and hypointensity on fast imaging employing steady- state acquisition (FIESTA) (D) differentiates the epidermoid from an arachnoid cyst.
- 117. Internal auditory canal (IAC) lipoma. A hyperintense lesion (black arrow— A) in the anterior aspect of the right IAC is seen on noncontrast T1- weighted magnetic resonance image. FLAIR with fat saturation completely suppresses signal from the lesion, confirming lipoma (white arrow—B).
- 118. Development of Solitary Plasmacytoma in the Internal Auditory Canal and Inner Ear after Allogeneic Hematopoietic Stem Cell Transplantation for Plasma Cell Leukemia.
- 119. A glomus jugulare tumour is a paraganglioma of the head and neck that is confined to the jugular fossa. While it is a rare tumour, it is the most common of the jugular fossa tumours. The lesion is arising from the 9th and 10th nerves and most common of middle ear. The unique names is according to the location: Jugular bulb- Glomus jugulare. Middle ear- Glomus tympanicum. Carotid body- Carotid body tumour. Vagus nerve- Glomus vagale. Clinical presentation: Pulsating tinnitus with conductive hearing loss,, Invasion of the cochlea, lead to sensorineural hearing loss. Otoscopy shows blue tympanic membrane.
- 120. Radiographic features CT: CT is most useful at assessing the bony margins of the tumour, which are typically irregularly eroded with a moth-eaten pattern. Eventually as the tumour enlarges the jugular spine is eroded and the mass extends into the middle ear, as well as inferiorly into the infratemporal fossa. CT is excellent at assessing the integrity of the ossicles and bony labyrinth . MRI T1 - low signal T2 - high signal T1 C+ (Gd) - marked intense enhancement Salt and pepper appearance is seen on both T1 and T2 weighted sequences; the salt representing blood products from hemorrhage or slow flow and the pepper representing flow voids due to high vascularity. DSA - angiography Angiography demonstrates an intense tumour blush, with the most common feeding vessel being the ascending pharyngeal . Early draining veins are also noted due to intra-tumoural shunting . Nuclear medicine Indium-111 labelled octreotide accumulates in these tumours due to the presence of receptors for somatostatin, best visualized with SPECT, but requires the tumour to be greater than 1.5cm in diameter.
- 121. Glomus tympanicum
- 122. Glomus jugulare. A mass is present in the jugular foramen (black asterisks). It is hypointense on T1-weighted magnetic resonance image (T1W MRI) (A), and hyperintense on T2-weighted magnetic resonance image (T2W MRI) (B), and enhances dramatically on postcontrast T1W MRI (C). Note the anterior displacement of the carotid flow void (white arrows) and a large flow void posteriorly (black arrows) within the tumor. Axial computed tomography (D) shows irregular bony erosion extending into the petrous portion of carotid artery canal (white arrowhead). Note the vertical segment of the facial nerve just lateral to the tumor (black arrowhead).
- 123. Glomus jugulare
- 124. Bony tumour related to the inner ear Fibrous dysplasia of bone is a fibro-osseous tissue disease which has unknown etiology and characterized by replacement of normal bone by a variable amount of fibrous tissue and woven bone. The disease may be unifocal, multifocal or as seen in McCune Albright Syndrome. Fibrous dysplasia rarely involves temporal bone and diagnosis is made with the displacement of neighboring structures. The aim of treatment is cosmetic and functional. Osteochondroma: An abnormal, solitary, benign growth of bone and cartilage, typically at the end of a long bone. Osteochondromas are usually discovered in persons 15 to 25 years of age and are the most common benign bone tumor. An osteochondroma is rarely occur at the ear.
- 126. Fibrous dysplasia affecting the ossicles and facial nerve canal.
- 127. Aneurysmal bone cyst of the temporal bone
- 128. Osteochondroma
- 129. Metastasis of the inner ear. Metastasis of the inner ear is usually hematogenous dissemination from mammary carcinoma, renal cell carcinoma and bronchogenic carcinoma as being three most common tumours this embolic type of metastasis. The second is direct invasion by nearby tumour such as those of the epipharynx and the parotid gland via perineural spread. Tumour cells occupy the internal auditory canal invading the V11th and V111 nerve trunks. Features of perineural spread: 1- Enlargement and enhancement of the involved nerve. 2- Obliteration of the fat surrounding neural foramina. 3- Atrophy of the muscles and replacement by fat of the involved nerve.
- 130. Esthesioneuroblastoma. A 39-year- old man presented with 1 month of decreased vision, left facial numbness, and swelling. Physical examination demonstrated left- sided exophthalmos and blindness. He was also unable to smell. Contrast-enhanced T1-weighted MRI demonstrated a large lesion that originated in the paranasal sinuses and extended through the cribriform plate into the anterior cranial fossa.
- 131. Perineural spread: facial nerve acinic cell carcinoma of left parotid gland. (A) Preoperative MRI – acinic cell carcinoma (solid arrow) with cranial nerve VII perineural spread (open arrow). (B) Postoperative MRI – skull base resection (open arrow), postoperative changes (closed arrow). Patient underwent parotidectomy and temporal bone resection. The proximal skull base surgical margin was clear but close (1 mm).
- 133. Metastasis. Ax T2WI(A) reveals area of inhomogeneous high signal filling the right PA, post gadolinium Ax/CorT1WI (B;C) show diffuse CE. Notice adjacent enhancing fat of the clivus and of VIII c.n (arrow in C).
- 134. Langerhans cell histiocytosis. Ax CT shows destructive bilateral PA masses with permeative bone changes (A). After steroid treatment, 2 years later, notice the complete healing.
- 135. Thank You.