Radiological Imaging of Large Bowel Diseases and Congenital Anomalies
•Download as PPTX, PDF•
46 likes•7,887 views

This document discusses congenital anomalies and diseases of the large bowel. It begins by describing congenital abnormalities that can cause obstruction in neonates and the importance of radiological imaging to diagnose the location and cause. It then discusses different types of intestinal obstructions and how radiography and contrast enema exams are used to further evaluate obstructions and make a specific diagnosis. Examples of different congenital anomalies and diseases seen on imaging are also presented, including colonic atresia, meconium ileus, Hirschsprung disease, and colon cancer.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Radiological Imaging of Large Bowel Diseases and Congenital Anomalies
Similar to Radiological Imaging of Large Bowel Diseases and Congenital Anomalies (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Recently uploaded
Recently uploaded (20)
Radiological Imaging of Large Bowel Diseases and Congenital Anomalies
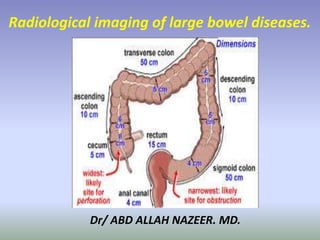
- 1. Dr/ ABD ALLAH NAZEER. MD. Radiological imaging of large bowel diseases.
- 2. Congenital Anomalies of the large bowel loops. Congenital abnormalities involving the large bowel lops are detected in neonates only when they are the direct cause of obstruction. Such abnormalities must be rectified surgically if the patient is to survive. Clinical signs and symptoms including abdominal distention, vomiting, and obstipation prompt the clinician to consult the radiologist, who must determine the presence, location, and cause of an obstruction. The diagnosis of obstruction is based on some interruption in this dispersion of air. Delayed passage of gas through the neonatal gut may occur as a result of traumatic delivery, septicemia, hypoglycemia, or brain damage. Absence of gas in the bowel may be noted in neonates with severe respiratory distress who are undergoing mechanical ventilation and in cases of continuous nasogastric suction.
- 3. Radiographyis the most valuable means of determining whether obstruction is present. This modality is often diagnostic; even if it is not, however, it may help determine the next most useful diagnostic procedure. Congenital anomalies causing incomplete obstruction (eg, stenoses, webs, duplications, malrotations, peritoneal bands, aganglionosis) may not manifest until later in life, and other types of examinations (eg, barium enema studies, ultrasonography [US], computed tomography [CT], magnetic resonance [MR] imaging) are generally needed for diagnosis. In this article, we discuss the importance of pediatric radiation protection and various means of ensuring adequate protection. We also discuss and illustrate a variety of congenital anomalies affecting the small bowel, colon, and rectum; evaluate the efficacy of various imaging modalities in the diagnosis and management of these conditions; and discuss the embryologic and pathologic basis of radiologic findings in appropriate cases as well as differential diagnoses and diagnostic pitfalls.
- 4. Neonatal intestinal obstructions may be classified as high or low. Obstructions occurring proximal to the mid ileum are called high or upper intestinal obstructions, whereas those involving the distal ileum or colon are called low intestinal obstructions. The distinction is critical because children with high obstructions usually need little or no further radiologic evaluation after radiography, and the specific diagnosis is made at surgery. Neonates with low obstructions require a contrast enema examination, which frequently provides a specific diagnosis and may be therapeutic. Low intestinal obstruction is defined as an obstruction that occurs in the distal ileum or colon. Signs include large bowel obstruction with vomiting, abdominal distention, and failure to pass meconium. In neonates, the differential diagnosis includes ileal and colonic atresia, meconium ileus or peritonitis, Hirschsprung disease, and functional immaturity of the colon. Anorectal malformations are also an important cause of low intestinal obstruction but are almost always evident at physical examination. The diagnosis of low obstruction is usually apparent at abdominal radiography because of the presence of many dilated intestinal loops, but the differentiation between ileal and colonic obstruction is difficult if not impossible. This distinction can readily be made with a barium enema study, which helps determine the presence of microcolon, indicates the position of the cecum with regard to possible malrotation, and shows the level of the obstruction in colonic atresia.
- 5. Colonic atresia. (a) Radiograph shows distended loops of bowel similar to those seen in low small bowel obstruction. (b) Image from a barium enema study demonstrates microcolon with complete obstruction to the retrograde flow of barium in the transverse portion of the colon.
- 6. Meconium ileus. (a) Abdominal scout radiograph shows marked distention of the small bowel and a “soap bubble” appearance in the right side of the abdomen (arrows), a finding suggestive of mottled air and feces. (b) US image shows dilated, fluid-filled intestinal loops containing echogenic material (calcified meconium) (arrows). Associated ileal atresia was seen at surgery.
- 7. Hirschsprung disease in a 6-month-old infant with a history of chronic constipation. (a, b) Frontal (a) and lateral (b) images from a barium enema study show the proximal sigmoid colon and descending colon as greatly dilated compared with the distal colon and rectum.
- 8. Total colonic aganglionosis. (a, b) Frontal (a) and lateral (b) images from a barium enema study show irregularity in the caliber of the colon with fewer redundant flexures than normal.
- 9. Meconium plug syndrome. (a) Image from a barium enema study shows a normal-sized rectum and colon with inspissated meconium filling defects (arrows). (b) Gross specimen shows the colon (C) and the typical appearance of an evacuated plug (arrows).
- 10. Malrotation. On an image from a barium enema study, the intestine occupies an intermediate position between that of nonrotation and the normal postnatal position. The cecum and the terminal ileum are displaced upward and medially.
- 11. Cystic communicating duplication of the colon in a 54-year-old woman with abdominal pain. Abdominal radiograph shows a round collection of air near the ascending colon (arrows).
- 12. Imperforate anus. Lateral radiograph shows an imperforate anus below the “M” line drawn through the junction of the upper two-thirds and lower one-third of the ischium (perineal surgical approach). (19) Ectopic anus. Voiding cystogram demonstrates a recto- urethral fistula (arrow). (20) Imperforate anus. Lateral voiding cystogram demonstrates an air-filled distal rectal pouch (arrows) ending blindly below the “M” line, a finding indicative of a low lesion. There is no fistula opening in the terminal bowel.
- 13. Benign tumours of the colon. Benign colorectal polyps About half of adults over the age of 40 develop lumps of tissue called polyps that grow from the inner lining (mucosa) of the colon or rectum. In most people, it is unclear how or why polyps develop. Polyps may look like a mushroom with a head and a stalk (pedunculated polyps). They may also be flat and grow along the inner surface of the wall of the colon or rectum (sessile polyps). Most polyps are non-cancerous (benign), but some do have the potential to become cancerous (malignant). Benign colorectal polyps are more common in men than women. The most common type of benign polyp is hyperplastic polyp. Hyperplastic polyps are usually less than 0.5 cm in diameter and most commonly occur in the rectum and sigmoid colon. There are several other types of benign polyps. The following benign polyps are much less common than hyperplastic polyps: inflammatory polyps (pseudopolyp) usually associated with chronic inflammatory bowel diseases such as Crohn's disease or ulcerative colitis.
- 14. Hamartomas contain normal cells that have an abnormal arrangement. Juvenile polyps also called retention polyps that contain many mucous glands usually occur as a single large polyp mostly found in children under 10 years of age. lipomas develop within the fat cells in the colon. Lymphoid polyps contain lymphoid cells, a type of white blood cell. Signs and symptoms Benign colorectal polyps usually do not have any symptoms. They are usually found during colorectal screening tests or investigation of other unrelated conditions. If symptoms are present, they may include: Bleeding from the rectum. Bloody stools. Fatigue (caused by anemia). Abdominal pain.
- 15. Diagnosis If the signs and symptoms of colorectal polyps are present, or if the doctor suspects colorectal polyps, tests will be done to make a diagnosis. Tests may include: digital rectal examination (DRE) double-contrast barium enema fecal occult blood test (FOBT) sigmoidoscopy colonoscopy virtual colonoscopy
- 16. Colonic polyp
- 17. Colonic polyp
- 18. Adenoma (arrow) in the sigmoid colon
- 19. Contrast-enhanced CT scans of the abdomen show ulcer encased by the mesenteric fatty tissue a mimicking colonic lipoma in the middle transverse colon
- 20. Colonic lipoma
- 21. Multiple polyps
- 25. Shwannoma of ascending colon.
- 26. Colon cancer is cancer of the large intestine (colon), the lower part of your digestive system. Rectal cancer is cancer of the last several inches of the colon. Together, they're often referred to as colorectal cancers. Most cases of colon cancer begin as small, noncancerous (benign) clumps of cells called adenomatous polyps. Over time some of these polyps become colon cancers. Polyps may be small and produce few, if any, symptoms. For this reason, doctors recommend regular screening tests to help prevent colon cancer by identifying polyps before they become colon cancer. Colon cancer. Symptoms Many cases of colon cancer have no symptoms. The following symptoms may indicate colon cancer: Abdominal pain and tenderness in the lower abdomen Blood in the stool Diarrhea, constipation, or other change in bowel habits Narrow stools. Weight loss with no known reason.
- 32. Large carcinoma of the sigmoid colonDistal transverse colon carcinoma.
- 33. Sigmoid carcinoma with apple core appearance.
- 35. Cecal mass
- 36. CT of lower abdomen shows a large mass (black arrows) encasing the colon (white arrow) near the junction of the descending and sigmoid portions.
- 37. Carcinoma of the ascending colon.
- 40. Two cases of transverse and descending Colon.
- 41. Adenocarcinoma in the right hepatic flexure with liver metastasis.
- 42. Mass at the ascending colon.
- 43. Distended large bowel loops, up to the distal descending colon where a well-defined mass at the descending colon.
- 44. Metastasis from carcinoma of the uterine cervix.
- 45. Thank You.