Presentation1.pptx, radiological imaging of pulmonary infection.
•Download as PPTX, PDF•
56 likes•10,515 views


Recommended
More Related Content
What's hot
What's hot (20)
Similar to Presentation1.pptx, radiological imaging of pulmonary infection.
Similar to Presentation1.pptx, radiological imaging of pulmonary infection. (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Recently uploaded
Recently uploaded (20)
Presentation1.pptx, radiological imaging of pulmonary infection.
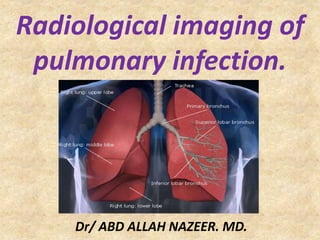
- 1. Radiological imaging of pulmonary infection. Dr/ ABD ALLAH NAZEER. MD.
- 9. Radiological Imaging: Chest x-ray : An x-ray exam will allow your doctor to see your lungs, heart and blood vessels to help determine if you have pneumonia. When interpreting the x-ray, the radiologist will look for white spots in the lungs (called infiltrates) that identify an infection. This exam will also help determine if you have any complications related to pneumonia such as abscesses or pleural effusions (fluid surrounding the lungs). CT of the lungs: A CT scan of the chest may be done to see finer details within the lungs and detect pneumonia that may be more difficult to see on a plain x-ray. A CT scan also shows the airway (trachea and bronchi) in great detail and can help determine if pneumonia may be related to a problem within the airway. A CT scan can also show complications of pneumonia, abscesses or pleural effusions and enlarged lymph nodes. Ultrasound of the chest : Ultrasound may be used if fluid surrounding the lungs is suspected. An ultrasound exam will help determine how much fluid is present and can aid in determining the cause of the fluid. MRI of the chest : MRI is not generally used to evaluate for pneumonia but may be used to look at the heart, vessels of the chest and chest wall structures. If the lungs are abnormal because of excess fluid, infection or tumor, an MRI may provide additional information about the cause or extent of these abnormalities.
- 13. RML Pneumonia
- 16. Right lower lobe pneumonia.
- 17. Left upper lobe pneumonia.
- 18. Right middle lobe pneumonia with hepatization.
- 19. Atypical Bacterial Pneumonia. Pneumonia is predominantly a clinical syndrome. The classic etiologic agents of atypical pneumonia are Legionella species, Mycoplasma pneumoniae, and Chlamydia pneumoniae. Many other diseases, caused by various pathogens, should be considered in the differential diagnosis. Such etiologic agents include fungi, mycobacteria, parasites, and viruses (e.g., influenza virus, adenovirus, respiratory syncytial virus, human parainfluenza virus, measles, varicella zoster, Hantavirus). In immunosuppressed patients, outbreaks of isolated cases of respiratory virus infections with atypical presentations are reported. These infections can be severe and may have concomitant bacterial etiologies. In endemic areas, certain zoonotic infections should be considered when patients present with atypical pneumonia. Noninfectious etiologies must be considered in atypical and non- resolving pneumonias.
- 21. Atypical severe Legionella pneumonia at lower lobes.
- 22. Atypical Chlamydia pneumonia of right upper and lower lobes.
- 23. Pneumonia caused by Mycoplasma pneumoniae.
- 25. Bilateral interstitial Influenza pneumonia.
- 26. Right-middle-lobe infiltrate in a 2-month-old boy with pneumonia due to respiratory syncytial virus
- 27. Pneumonia, Viral
- 28. 2 cases of Interstitial Pneumonia
- 29. CT scan showing bronchiolitis obliterans organizing pneumonia Cryptogenic-organizing-pneumonia.
- 30. Pneumocystis pneumonia (PCP) is an atypical pulmonary infection and the most common opportunistic infection in patients with acquired immunodeficiency syndrome (AIDS).
- 35. Left lingular Round pneumonia.
- 36. Left lung round pneumonia.
- 37. Left lower lobe round pneumonia.
- 42. Radiographic features Plain film Bronchopneumonia is characterised by multiple small nodular or reticunodular opacities which tend to be patchy and confluent. This represents areas of lung where there are patches of inflammation separated by normal lung parenchyma . The distribution is often bilateral and asymmetric, and predominantly involves the lung bases. CT - HRCT chest Multiple foci of opacity can be seen in a lobular pattern, centred at centrilobular bronchioles. These foci of consolidation can overlap to create a larger heterogeneous confluent area of consolidation. This may result in a tree-in-bud appearance.
- 43. 2 Cases of bilateral bronchopneumonia.
- 44. 2 Cases of bilateral bronchopneumonia.
- 47. Bronchopneumonia
- 49. Bronchopneumonia show consolidation and ground-glass opacity distributed heterogeneously in the lungs.
- 50. A child with bilateral bronchopneumonia.
- 54. Left upper lobe lung abscess.
- 55. Right lower lobe lung abscess.
- 56. Right upper lobe lung abscess.
- 57. Left upper lobe lung abscess.
- 58. Left upper lobe lung abscess with pleural effusion.
- 59. Right upper lobe lung abscess with left pleural empyema.
- 60. Thank You.