Presentation1.pptx, radiological vascular anatomy of the chest and abdomen.
•Download as PPTX, PDF•
81 likes•10,286 views


Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to Presentation1.pptx, radiological vascular anatomy of the chest and abdomen.
Similar to Presentation1.pptx, radiological vascular anatomy of the chest and abdomen. (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Presentation1.pptx, radiological vascular anatomy of the chest and abdomen.
- 1. Radiological vascular anatomy of the chest and abdomen. Dr/ ABD ALLAH NAZEER. MD.
- 10. Coronary anatomy. On the left an overview of the coronary arteries in the anterior projection. Left Main or left coronary artery (LCA) Left anterior descending (LAD) diagonal branches (D1, D2) septal branches Circumflex (Cx) Marginal branches (M1,M2) Right coronary artery Acute marginal branch (AM) AV node branch Posterior descending artery (PDA)
- 11. On the left an overview of the coronary arteries in the right anterior oblique projection. Left Main or left coronary artery (LCA) Left anterior descending (LAD) diagonal branches (D1, D2) septal branches Circumflex (Cx) Marginal branches (M1,M2) Right coronary artery Acute marginal branch (AM) AV node branch Posterior descending artery (PDA)
- 12. Left Coronary Artery (LCA). The left coronary artery (LCA) is also known as the left main. The LCA arises from the left coronary cusp. The aortic valve has three leaflets, each having a cusp or cup-like configuration. These are known as the left coronary cusp (L), the right coronary cusp (R) and the posterior non-coronary cusp (N). Just above the aortic valves there are anatomic dilations of the ascending aorta, also known as the sinus of Valsalva. The left aortic sinus gives rise to the left coronary artery. The right aortic sinus which lies anteriorly, gives rise to the right coronary artery. The non-coronary sinus is positioned on the right side. The LCA divides almost immediately into the circumflex artery (Cx) and left anterior descending artery (LAD). On the left an axial CT-image. The LCA travels between the right ventricle outflow tract anteriorly and the left atrium posteriorly and divides into LAD and Cx.
- 13. RCA, LAD and Cx in the anterior projection.
- 14. RCA, LAD and Cx in the right anterior oblique projection
- 15. RCA, LAD and Cx in the lateral projection.
- 16. CT image of the LAD in RAO projection LAD in RAO projection.
- 17. Circumflex and LAD seen in Lateral projection.
- 18. RCA, LAD and LCx in Anterior projection.
- 19. Curved MPR (Fig. 1A), MIP (Fig. 1B), and VRT (Fig. 1C) images demonstrate the LAD with mild stenosis (arrows) from soft plaque, and a myocardial bridge (arrowheads) in the middle LAD with no evidence of stenosis. The Cx (dashed arrow) and the RCA (double arrows) appear to be normal, although the Cx is small in caliber.
- 20. CT angiography with eliminated contrast filled left ventricle entire coronary artery anatomy.
- 21. Conventional “Angio-like view” using CT technology.
- 23. Multiplanar reconstructions of the coronary arteries.
- 24. CT Scan of the thoracic aorta, heart and great vessels. Great vessels.
- 25. Aortic arch
- 27. Atria
- 28. Ventricles.
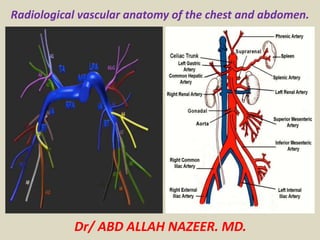
- 34. Radiological vascular anatomy of the vascular anatomy of the abdomen. Celiac axis (trunk, artery) a. First unpaired branch off abdominal aorta (~ L-1). b.Originates from ventral surface. c. Gives rise to splenic, common hepatic, & left gastric arteries.
- 35. Celiac Artery a. First unpaired branch of abdominal aorta (~T-12) b. Gives rise to: 1. Splenic Artery: a. largest on left b. supplies spleen, pancreas fundus of stoma
- 36. CT angiogram abdominal vessels anatomy.
- 37. Arteries of the Abdominal Aorta.
- 38. Celiac artery
- 39. Celiac artery.
- 43. Common Hepatic Artery a.Right branch of celiac a. b. Continues to GDA, then. Proper Hepatic Artery a.Branches within liver b.Begin at ~porta hepatis
- 44. Blood Supply to Liver.
- 45. Superior Mesenteric Artery a. Second, unpaired branch of abdominal aorta. b. Originates ~ lower L-1 body. c. 1 – 2 cm below celiac axis. d. Supplies small intestines, pancreas, omentum, ascending and transverse colon.
- 46. SMA a. Second unpaired branch b. Arises 1 – 2 cm below celiac artery c. May have common origin d. After ~6”, 1. courses parallel to aorta 2. then turns oblique toward right iliac fossa Numerous branches that sometimes anastomose e.Supplies: 1. small intestines 2. cecum 3. appendix 4. ascending & transverse colon. 5. pancreas
- 49. Coronal maximum intensity projection of the superior mesenteric artery and its branches. This image was created on a workstation with CT data from a state-of-the-art 16-slice multidetector CT scanner. Note the fine detail that is visible of the end-organ arteries of the jejunum and ileum.
- 51. Inferior Mesenteric Artery a.Arises just above the bifurcation of the aorta (~L-3/4) b. Last unpaired branch of aorta c. Supplies jejunum, descending and sigmoid colon, rectum
- 52. Distribution of the Superior and Inferior Mesenteric Arteries
- 54. Renal arteries a. First major paired branches from aorta. b. Arise opposite each other 1-2 cm below SMA (L-2). c. Multiple renal arteries occur in 20% of patients.
- 56. Renal Arteries.
- 58. Normal renal arteries. Axial MIP image, obtained to evaluate for renal artery stenosis, clearly shows the renal arteries (arrows), which are normal and demonstrate no evidence of stenosis.
- 59. MIP of the renal arteries.
- 60. Volume Rendering images demonstrate the normal anatomy of renal arteries (arrows). The renal arteries typically arise from the aorta at the level of L1, L2 intervertebral disc below the origin of the superior mesenteric artery (arrowhead).
- 61. Coronal volume rendering images show anterior (A)and posterior (B) views of normal segmental anatomy of the renal artery. The first division is the posterior branch (arrow head). Posterior branch gives two segmental branches (black arrows), supplying the posterior central portion of the kidney. The main renal artery then continues its course before branching into four anterior branches(arrows)at the renal hilum.
- 62. Coronal(A) and axial (B) volume rendering images shown or mal renal vein anatomy. Renal veins(arrows)course anterior part of the renal arteries(arrowheads).The left renal vein normally courses between the SMA (thin arrow) and the aorta (small asterisk) before draining into the medial aspect of the inferior vena cava (big asterisk), while the right one from the lateral aspect.
- 63. Inferior Vena Cava a.Formed at ~ L-5 b.by union of Common Iliac Veins c.Largest vein in body d.Dilation may be due to: 1.right-sided CHF 2.Portal hypertension
- 64. Major Veins of the Abdomen.
- 65. Veins of Portal Circulation a.SMV: joins with splenic vein. 1.runs parallel to SMA. 2.On right side of abdomen. b.IMV: terminates in splenic vein. c.Portal Vein: enters liver.
- 66. Veins of the Hepatic Portal System.
- 72. Axial CT images at L4/L5 level in portal fase and MIP angio TC reconstruction. Note how the abdominal aorta divides into common iliac arteries at L4-L5 level and how after these division these vessels run anterior iliac veins and inferior to vena cava
- 73. Axial CT images at S2 level showing distal pelvic vessels. The common iliac arteries divide, at the level of L5-S1, into two branches, the external and internal iliac (hypogastric) arteries. The external iliac artery supplies the lower extremity, while the hypogastric artery supplies the pelvic viscera and muscles of the pelvis.
- 74. Major branches of the abdominal aorta.
- 75. Thank You.