Presentation1.pptx, ultrasound examination of the hip joint
•Download as PPTX, PDF•
80 likes•10,216 views


Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Presentation1.pptx, ultrasound examination of the hip joint
Similar to Presentation1.pptx, ultrasound examination of the hip joint (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Presentation1.pptx, ultrasound examination of the hip joint
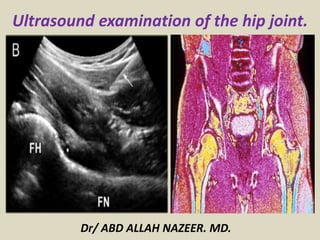
- 1. Ultrasound examination of the hip joint. Dr/ ABD ALLAH NAZEER. MD.
- 2. ANTERIOR HIP •sartorius and tensor fasciae latae muscles •rectus femoris muscle •iliopsoas muscle •femoral neurovascular bundle •coxo-femoral joint MEDIAL HIP • adductor tendons and muscles LATERAL HIP • gluteus tendons and muscles POSTERIOR HIP ischio crural tendons (hamstrings) sciatic nerve. The hip joint anatomy can be subdivided into four compartments, each of those including a group of structures that are extremely important for hip stability.
- 3. The ultrasound scan shows the tendinous insertions of sartorius (Sa) and tensor fasciae latae (TFL) muscles on the antero-superior iliac spine (SIAS).
- 4. The axial scan shows the tendinous insertion of rectus femoris (arrowheads) into the SIAI. Ps= iliopsoas muscle; SIAI= Anterior-Inferior Iliac Spine
- 5. The ultrasound scan shows the tendinous insertion of rectus femoris (arrowheads) onto the AIIS. RF= muscle belly of rectus femoris ; Ps= psoas muscle; SIAI= Anterior-Inferior Iliac Spine.
- 6. Axial evaluation of direct (arrowheads) and indirect (asterisk) tendons of rectus femoris muscle. Sa= sartorius; F= femur.
- 7. The axial scan shows the distal tendinous aponeurosis (arrowhead) of rectus femoris muscle (RF) shaped like a "C". Vi= vastus intermedius muscle; F= femur.
- 8. The axial scan shows the femoral neurovascular bundle: femoral artery (Af), femoral vein (Vf) and femoral nerve (Nf). Pe= pectineus muscle
- 9. The scan shows the femoral head (F) covered by the articular cartilage, the acetabulum (Ac), the acetabular labrum (asterisk), and the anterior capsular profile (empty arrowheads). Ps= psoas muscle.
- 10. The longitudinal scan shows the tendon insertion (asterisk) of adductor longus (AL), adductor brevis (AB) and adductor magnus (GA) muscles in correspondence of the pubic symphysis.
- 11. The axial scan shows the tendinous insertion of gluteus minimus (asterisk). medius @ and maximus # into the femoral greater trochanter (GT). Arrowheads= tensor fasciae latae tendons.
- 12. Coronal Scan Plane. The gluteus minimus and medius insert into the greater trochanter.
- 13. Transverse Scan Plane Transverse view of the gluteus Minimus and gluteus Medius Tendons.
- 14. The longitudinal scan shows the tensor fasciae latae tendon (arrowheads) superficial to the greater trochanter (GT).
- 15. The axial scan shows the tendinous insertion of long head of biceps femoris (1), semitendinosus (2) and semimembranosus (3) muscles. Ti= ischiatic tuberosity.
- 16. The longitudinal scan shows the tendinous insertion (asterisk) of semitendinosus (St) and semimembranosus (Sm) into the ischiatic tuberosity (Ti).
- 17. The axial scan shows the sciatic nerve, according to its short-axis.
- 28. Ultrasound is a valuable diagnostic tool in assessing the following indications; Developmental dysplasia of the hip Muscular, tendinous and some ligamentous damage (chronic and acute) Bursitis Joint effusion Vascular pathology Haematomas Soft tissue masses such as ganglia, lipomas Classification of a mass e.g solid, cystic, mixed Post surgical complications e.g abscess, edema Guidance of injection, aspiration or biopsy Some boney pathology.
- 29. Developmental Dysplasia of the Hip (DDH). Developmental dysplasia of the hip is an abnormal formation of the hip joint in which the ball at the top of the thighbone (femoral head) is not stable in the socket (acetabulum). The hip is a ball and socket joint, and dysplasia can refer to a hip that is subluxatable (unstable if stressed), dislocatable (can come out of socket under stress), or currently dislocated. The severity of instability or looseness varies in each patient. Newborns and infants with DDH may have the ball of his or her hip loosely in the socket, or the hip may be completely dislocated at birth. Developmental dysplasia of the hip (DDH) may occur during fetal development, at delivery, or after birth. Causes Hip Dysplasia/DDH? The exact cause of DDH is unknown, but research has discovered several theories and risk factors for hip dysplasia. The four F's of DDH: First born Female Foot First (breech) Family history
- 30. Hip ultrasounds are used to detect DDH in newborns and young infants. The ultrasound can accurately determine the stability of the hip joint, and can be useful in the diagnoses and management of DDH. By using high frequency sound waves, there is no risk of radiation exposure to the baby. Because many of the bones making up the hip joint are made of soft cartilage, not hard bone, plain x-rays are generally not helpful until the baby is 5-6 months old. Ultrasound enables direct imaging of the cartilaginous portions (bones that are not yet ossified) of the hip that cannot be seen on plain radiographs.
- 31. Morin index. Schematic representation of Graf classification.
- 33. Anatomic schematic interpretation of the standard coronal plane. S, superior planes; L, lateral(superficial)planes; FH, femoral head.
- 34. Coronal view. c- capsule; G- gluteus muscles; H- cartilaginous femoral head; IL – ilium: IS- Ischium; L- labrum; LT- ligamentum teres; Tr-triradiate cartilage. Morin Index - In this infant the Morin index is normal (10/16.6 60%).
- 35. Measure of α and β angles – type I hip. Schematic and ultrasound coronal scan with alpha and beta angle calculation.
- 36. Coronal ultrasound image of the left hip. Normal type I hip (alpha angle > 60 degrees).
- 37. Normal mature hip. Type Ib according to Graf (α= 65°, β= 74°); angular bony promontory (arrow); IL, ilium; TC, hypoechoic triradiate cartilage; 1, Baseline; 2, acetabular roof line; 3, Labral line; (*), hyaline cartilage of the acetabular roof; (+), labrum.
- 38. A, B. Same hip. Physiological immature hip, appropriate for age. Type IIa(+) according to Graf (α= 55°, β= 77°); rounded bony promontory (arrow); FH, femoral head; GT, great trochanters; IL, ilium; TC, hypoechoic triradiate cartilage; 1, Baseline; 2, acetabular roof line; 3, Labral line; (*), hyaline cartilage of the acetabular roof; (+), labrum.
- 39. Coronal ultrasound image of the left hip. Type IIa hip (alpha angle of 50-59 degrees).
- 40. Critical hip. Type IIc according to Graf (α= 44°, β= 74°); Rounded or flattened bony promontory; FH, femoral head; GT, great trochanters; TC, hypoechoic triradiate cartilage.
- 41. Coronal ultrasound image of the right hip. Type III with decentering of the femoral head (alpha angle < 43 degrees).
- 42. Graf type IIIb (α= 34°, β= 123°).
- 43. Graf type IV
- 44. Type IV hip – the femoral head is totally out the acetabular cup and is not aligned with the acetabulum
- 46. Joint Effusion: Inflammatory joint diseases, such as rheumatoid arthritis and septic arthritis, are often accompanied by joint effusion. In healthy adults on the other hand hip joint effusion is very uncommon. The prevalence in less severe, or early stage hip disorders is, however, not well documented. We neither know which symptoms nor signs in early or less severe hip disorders relate to joint effusion. Ventral Hip sonography: Depiction of the right and left hips in comparison: obvious echo-free joint effusion on the left with distancing of the capsule
- 47. Coxitis with an effusion in the anterior recess and slight hypervascularity.
- 48. Irritable hip on the right side with effusion in the anterior recess of the hip.
- 49. Hip joint effusion and minimal synovial thickening.
- 50. Trochanteric bursitis is inflammation of the bursa (a small, cushioning sac located where tendons pass over areas of bone around the joints), which lies over the prominent bone on the side of your hip (femur). The superficial trochanteric bursa is located over the greater trochanter. This is the most commonly inflamed bursa. A deep trochanteric bursa lies deeper and can become inflamed in more severe cases. Causes Trochanteric Bursitis? The trochanteric bursa may be inflamed by a group of muscles or tendons rubbing over the bursa and causing friction against the thigh bone. This injury can occur traumatically from a fall or a sport-related impact contusion. It can also be a case of gradual onset via a repetitive trauma to the bursa from such activities as running (with poor muscles control or technique), walking into fatigue, or cycling, especially when the bicycle seat is too high. It is also a secondary injury associated with chronic conditions such as: Scoliosis - curvature of the spine Unequal leg length Weak hip muscles Osteoarthritis (degenerative joint disease) of the hips or lower back Calcium deposition in the gluteal tendons that run over the bursa Rheumatoid arthritis.
- 51. Effusion in the anterior recess and filling of the iliopsoas bursa.
- 52. Iliopsoas bursa.
- 53. Iliopsoas bursitis with large fluid filled bursa.
- 54. Iliopsoas bursitis with increased vascularity of the bursal wall.
- 55. Iliopsoas bursitis with a large iliopsoas bursa with thickened synovium in a patient with a hip prosthesis.
- 56. Irritable hip – transient synovitis and reactive arthritis Irritable hip or transient synovitis (TS) is the most common cause of hip pain in the pediatric patient. TS . and reactive arthritis. are both benign, self limiting conditions. The temperature is usually normal or slightly raised, white cell count (WCC) and erythrocyte sedimentation rate (ESR) are normal or close to normal. Treatment is rest and analgesia. The addition of an anti- inflammatory may speed recovery. Usually these conditions follow a recent viral illness in particular an upper respiratory tract infection (URTI). Transient synovitis; hypoechoic effusion without hyperemia.
- 57. Patient with transient synovitis. Sagittal US image shows the superior articular recess (SAR) effusion (A) with small particles floating in the effusion (B).
- 58. Reactive arthritis, often bilateral.
- 59. Infectious arthritis is a painful infection in the joint. It may also be referred to as septic arthritis. It occurs when an infection, caused by a bacteria or virus, spreads to a joint or the fluid surrounding the joint (synovial fluid). This infection usually begins in another area of the body and spreads through the bloodstream to the joint tissue. The infection may also enter the body through surgery, open wounds, or injections. Infectious arthritis usually only occurs in one joint. Most often, the joint affected is a large joint such as the knee, hip, or shoulder. It occurs more often in children and older adults. Symptoms of infectious arthritis can vary depending on the individual’s age, as well as the medications the individual is taking. Symptoms may include: severe pain that worsens with movement swelling of the joint warmth and redness around the joint fever chills fatigue weakness decreased appetite rapid heartbeat irritability
- 60. Septic arthritis in the neonate Premature infants are at risk of infection. Regular intervention, in particular vascular access lines increases the risk of introduced infection. Premature babies have an immature immune system and do not exhibit obvious signs of sepsis. The prevalence of MRSA is increasing in hospital intensive care units. Neonates in intensive care units with septic arthritis are more likely to have MRSA infection than non-MRSA. Bony destruction can occur quickly. with a worse outcome than those with non-MRSA infection, due to the limited range of antibiotics effective in treating an MRSA infection and the relatively late presentation. Disruption of the epiphysis leads to arrest of growth of the upper femur with resultant leg length discrepancies Destruction of the head of femur leads to life long joint deformity. Early identification of joint sepsis aids early aggressive management, which increases the chance of retaining the use of the joint and limb.
- 61. Septic Arthritis of the right hip joint. Septations are seen within the fluid.
- 62. Pyorthritis of left hip joint.
- 63. Destruction of head of femur of left hip due to MRSA septic arthritis.
- 64. Septic arthritis with destruction of the head of the right hip and femur.
- 65. Juvenile idiopathic arthritis Hip involvement in juvenile idiopathic arthritis (JIA) tends to be bilateral and develops in 30–50% of children suffering from JIA. It is uncommon to have hip monoarthritis. Clinical examination and history usually suggest the diagnosis. Ultrasound may show a joint effusion and thickened synovium. These changes and other findings of joint destruction are often better seen on MRI or plain radiographs. Ultrasound can be used for image-guided intra-articular steroid injections.
- 66. Bilateral JIA with effusion.
- 67. Juvenile idiopathic arthritis with thickened synovium and joint effusion.
- 68. Hemoarthrosis of left hip joint. Hemoarthrosis is bleeding into a joint. It often causes inflammation and pain. Hemoarthrosis is more likely to occur in people with bleeding disorders, such as hemophilia (a rare inherited condition), or in those who use blood-thinning medication, such as warfarin. It also can develop after an injury to a joint when blood vessels in the joint are also injured.
- 69. Hemoarthrosis of left hip joint.
- 70. Slipped capital femoral epiphysis (SCFE) is an unusual disorder of the adolescent hip. It is not rare. For reasons that are not well understood, the ball at the upper end of the femur (thigh bone) slips off in a backward direction. This is due to weakness of the growth plate. Most often, it develops during periods of accelerated growth, shortly after the onset of puberty. The cause of SCFE is unknown. It occurs two to three times more often in males than females. A large number of patients are overweight for their height. In most cases, slipping of the epiphysis is a slow and gradual process. However, it may occur suddenly and be associated with a minor fall or trauma. Symptomatic SCFE, treated early and well, allows for good long-term hip function. Ultrasonography show in recent slipped epiphysis the ultrasound image revealed a step at the anterior physeal line(mean 6.4 mm), diminished distance between the anterior acetabular rim and the femoral metaphysis(mean 4.3 mm), and an joint effusion. As metaphyseal remodelling progressed the physeal step decreased. The femoral neck appeared straighter in hips which has been symptomatic for longer than three weeks.
- 71. Slipped capital epiphysis with effusion in the anterior recess
- 72. Slipped capital femoral epiphysis with joint effusion and posterior displaced epiphysis.
- 73. Slipped capital femoral epiphysis with joint effusion and posterior displaced left epiphysis.
- 74. Slipped capital femoral epiphysis with joint effusion and posterior displaced left epiphysis.
- 75. Legg-Calve Perthes’ disease Legg-Calve Perthes’ disease is an idiopathic avascular necrosis (AVN) of the hip joint. The peak incidence of LCP is between four and eight years of age with boys being effected more than girls. Recently LCP disease has been reported in children younger than two years of age and must be a differential diagnosis in any hip pain investigation of young children. Trauma to the hip joint can cause increased intra-osseus pressure and compression of blood vessels, this may lead to avascular necrosis. In advanced disease, radiographs will display the classic picture of a reduced height head of femur with fragmentation. In early LCP the radiograph may be normal. A joint effusion may accompany LCP. An underlying pathology should be suspected when a sustained effusion is present. In early LCP the head of femur may exhibit slight irregularity. The treatment for LCP, especially when diagnosed early, is rest.
- 76. Hip effusion. Comparison of both heads of femur demonstrates irregularity of left head of femur (LCP) as well as a joint effusion.
- 77. Hip effusion. Appreciation of possible head of femur irregularity more obvious in comparison to normal hip.
- 78. Ganglion of the hip is rare, or at least is rarely recognized. Embedded in muscles and covered by the femoral vessels and nerve, its hidden location accounts for the diagnostic difficulties which can cause varied clinical presentations. Ultrasonography, computed tomography (CT), and magnetic resonance imaging (MRI) help to rule out more frequent disorders of this region, but in some cases it is still detected only by surgery.
- 79. Right groin mass in a middle-aged woman with no recent history of trauma or instrumentation. (a, b) Color (a) and spectral (b) Doppler US scans are suggestive of venous flow (solid arrow in a) within a cystic right groin mass a provisional diagnosis of venous pseudoaneurysm was made
- 80. Thank You.