Presentation1.pptx, ultrasound examination of the orbit.
•Download as PPTX, PDF•
72 likes•8,644 views

Ultrasound examination of the orbit. The document provides information on: 1. Using ultrasound to examine the eye and identify normal anatomy and common pathologies. 2. Scanning techniques for assessing the anterior chamber, posterior chamber, and retro-ocular region. 3. Descriptions of common pathologies like vitreous hemorrhage, retinal detachment, choroidal melanoma, and more and how they appear on ultrasound. 4. Images demonstrating ultrasound findings for various eye conditions.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (14)
Similar to Presentation1.pptx, ultrasound examination of the orbit.
Similar to Presentation1.pptx, ultrasound examination of the orbit. (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Presentation1.pptx, ultrasound examination of the orbit.
- 1. Ultrasound examination of the orbit. Dr/ ABD ALLAH NAZEER. MD.
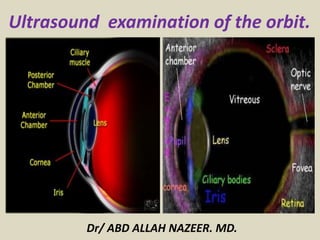
- 2. ULTRASOUND OF THE EYE: Normal ANATOMY OF THE EYE
- 3. External eye anatomy Cross sectional eye anatomy. Scan gently through a closed eye. The comparative anatomy between the eye ultrasound and the anatomy diagram above.
- 4. Eye ultrasound: Hover the cursor over to see highlighted anatomy of the anterior chamber Increase your depth to visualize the retro- occular region. View the eye with the patient looking to extremes of up, down, left and right.
- 5. ULTRASOUND OF THE EYE PROTOCOL ROLE OF ULTRASOUND Ultrasound is used primarily to assess internal structures of the globe, particularly when direct visualization is obscured by cataracts or hemorrhage. Assessment of intraocular masses & measurement of tumour thickness for staging. Differentiating between choroidal or retinal detachments. Some retro-occular applications. Relationship of normal anatomy and pathology to each other EQUIPMENT SELECTION Use of a high resolution, small footprint probe (10-15MHZ) is essential when assessing the internal structures of the globe. Good colour / power / Doppler capabilities when assessing vessels or vascularity of a structure.
- 6. SCANNING TECHNIQUE: Explain the procedure. Position the patient supine. Scan the patient through closed eyes. Give the patient some tissues and explain that should they need to open their eyes, to let you know and they can use the tissues to wipe their eye. If possible, use sterile gel. Apply a small amount of gel to the probe. Be prepared to change frequency output of probe (or probes) to adequately assess both superficial and deeper structures. ANTERIOR CHAMBER: Reduce the depth to include the posterior aspect of the lens and zoom to fill the screen. Use thick gel and minimal to no pressure because the anterior chamber is easily compressed. Sweep in both sagittal and transverse checking for symmetry. Look for sharp margins where the cornea meets the lateral margins of the iris & ciliary bodies. Ensure the lens is intact, anechoic and normally located. A cataract will be seen as echogenic heterogeneity of the lens. Document the normal anatomy and any pathology found, including measurements and vascularity if indicated.
- 7. POSTERIOR CHAMBER Increase the depth to include the entire globe and proximal optic nerve. In transverse, ask the patient to look left and right to facilitate maximum scan range. Similarly, in sagittal, ask the patient to look up/down. Look for a smooth inner wall of uniform thickness and echogenicity. Check for homogeneity of the vitreous tumour. Commonly in elderly people there will be some echogenic 'debris' within the vitreous due to degenerative changes. A vitreous hemorrhage will be seen as mobile, fibrinous, complex material possible tethered. Whilst rare to see pathology, check that the optic nerve is uniform and symmetrical in size bilaterally with no retro-occular masses. Document the normal anatomy and any pathology found, including measurements and vascularity if indicated.
- 8. COMMON PATHOLOGY Vitreous hemorrhage Retinal detachment Choroidal detachment Melanoma Lens replacement and pathology Foreign body and trauma Drusen Staphyloma
- 9. A vitreous hemorrhage. Bleeding can occur as a result of a ruptured microaneurism in diabetics (a small balloon-like protrusion from a weak area in a blood vessel), leakage from abnormal vessels in retinal vascular conditions, or from damage to the retina. Microaneurism usually occur in patients who have diabetic retinopathy. When the blood sugar is high, the blood vessels get damaged, causing localized weak areas. Over time, these weak areas start to protrude out, forming a microaneurism. When an aneurism bursts, blood enters into the vitreous, causing a vitreous hemorrhage. Abnormal vessels that grow in response to low oxygen levels in retinal vascular conditions (proliferative diabetic retinopathy, vein occlusions, etc) are very fragile and tend to leak. Sometimes these abnormal vessels grow from the retina into the vitreous cavity and leak blood, causing a vitreous hemorrhage. Mechanical damage to the blood vessels of the retina can occur from a retinal tear or trauma to the eye. Like any other part of the body, if a blood vessel gets damaged, it will start to bleed. If mechanical damage occurs to the retina, retinal blood vessels can get damaged and bleed into the vitreous cavity, causing a vitreous hemorrhage.
- 10. Who can get a vitreous hemorrhage and what are the risk factors? A vitreous hemorrhage can occur in anyone, though the incidence of occurrence is relatively small with only 7 cases per 100,000 people in the United States. Factors that increase the possibility of developing a vitreous hemorrhage include: 1. Age 2. Proliferative Diabetic Retinopathy 3. Retinal Tear 4. Retinal Vein Occlusion with proliferative retinopathy 5. Posterior Vitreous Detachment without a tear 6. Retinal Detachment 7. Trauma to the eye What are the symptoms of a vitreous hemorrhage? Depending on the severity of the vitreous hemorrhage a patient may not experience any symptoms, though this usually isn’t the case. Typically a patient will experience one or more of the following symptoms: 1. Decreased vision 2. Sensation of looking through hazy or smoke 3. Multiple new floaters 4. Cobweb shapes, dark streaks 5. Flashes of light
- 11. Vitreous Hemorrhage Ultrasound Vitreous hemorrhage.
- 12. Vitreous Hemorrhage Ultrasound Vitreous hemorrhage ultrasound.
- 14. RESOLVING VITREOUS HAEMORRHAGE ORGANISED VITREOUS HAEMORRHGAE
- 15. POSTERIOR VITREOUS DETACHMENT (PVD): Any derangement in the vitreous cavity leads to the detachment of the posterior vitreous from the retina. On the B mode, PVD is seen as a thin irregular membrane with distinct after-movements. The presence of after-movements is a hallmark of PVD. On A scan, PVD has low reflectivity and the reflectivity decreases as we go peripherally towards the ora-serrata. RETINAL DETACHMENT: Retinal detachment can be hematogenous (primary) or non- hematogenous (secondary to other pathologies, e.g. choroidal melanoma). On B scan, retinal detachment is seen as a highly reflective, V-shaped membrane attached to the optic disc (4) . This membrane classically has restricted mobility. On A scan, there is 100% reflectivity over its entire extent. It is very important to differentiate retinal detachment from a thick PVD attached to the optic disc.
- 16. Posterior Vitreous Detachment Ultrasound.
- 17. Ultrasound for Acute Retinal Detachment.
- 19. RETINAL DETACHMENTPOSTERIOR VITREOUS DETACHMENT (PVD).
- 21. Ultrasound image of the thin, hyperechoic retinal membrane detached and floating in the vitreous humor. Retinal detachment.
- 23. CHOROIDAL MELANOMA. CHOROIDAL MELANOMA Choroidal melanoma is the commonest tumor of the eye in the middle-age group. Melanomas on B scan are seen as dome shaped or collar button shaped tumour with the base over the choroid. The collar button shape is due to the break in the bruch`s membrane. The collar button shape is pathognomonic of melanoma. Melanomas are highly vascular tumours. The vascularity is seen as fast flickering motion within the tumour. This motion is more marked at the base of the tumour. Choroidal excavation may also be seen at the base of the tumour (6) . On A scan it has a very characteristic appearance - there is a high anterior surface spike followed by low internal reflectivity with typical cascading effect.
- 25. Choroidal typical melanoma. 6.a: A minimally raised lesion of approximately 5 mm in the posterior wall of the right eye , which corresponds to a melanoma (arrow). 6.b: Retinography of the same patient : the irregularly pigmented lesion corresponds to the melanoma 6.c: Angiography shows some areas of contrast enhancement corresponding to the melanoma 6.d: Optical coherence tomography showing a raised lesion developing minimal retinal detachment.
- 26. Amelanotic melanoma. 7.a: Raised polypoid lesion of about 6 mm proved to be an amelanotic melanoma. 7.b: Retinography of the patient shows the mass, round and shiny. 7.c: Angiographic study shows a strong contrast enhancement of the mass.
- 27. CHOROIDAL METASTASES CHOROIDAL METASTASES The commonest tumor metastazing of the choroid, is oat cell tumor of the lung in male and breast in the female. On B mode, metastasis is seen as an irregular lobulated mass arising from the choroid with multiple hypoechoic areas within it. On A scan, there is a very high irregular reflectivity because of multiple interfaces. Typically, metastatic lesions do not show any vascularity, either on A scans, or Doppler studies.
- 28. CHOROIDAL HAEMANGIOMA HAEMANGIOMA Choroidal hemangiomas may occur as solitary lesion or as part of Sturge-Weber syndrome. Choroidal haemangioma does not show increased vascularity. On B scan, choroidal haemangioma are seen as dome shaped choroidal mass lesion with a broad base. Choroidal haemangioma has irregular echotexture. The irregular echotexture is due to multiple interfaces within the tumour. A small calcific area is noted over the surface of choroidal haemangioma. This calcific area is a Phleboliths. It may or may not produce shadowing depending on the density of calcium within the phlebolith. The presence of phlebolith is diagnostic of haemangioma, but absence does not rule out haemangioma.
- 29. Ocular Trauma. Globe rupture. Dislocated lens. Retinal Detachment. Vitreous hemorrhage.
- 31. Globe rupture-moderate vitreous loss.
- 32. Globe Rupture.Retro bulbar Hematoma.
- 34. Ultrasound of lens Dislocation.
- 35. A hyperechoic foreign body (blue) in the eye.
- 37. Endophthalmitis. Ocular ultrasound (18 Hz) A) RE: increased echogenicity and the anteroposterior diameter of the anterior chamber (on physical examination by slit lamp showed hypopyon) and cataract. B) RE: anteroposterior diameter of anterior chamber: 0.27 cm. C) OI: anteroposterior diameter of anterior chamber 0.20 cm
- 38. Endophthalmitis. Ocular ultrasound (18 Hz) mode B and color Doppler. A) Images show increased anterior chamber, cataract, increased soft tissue of eyelid, vitreous membranes and heterogeneous echogenicity in the vitreous. B) Intense color Doppler in soft tissue of eyelid. C) Absence of color Doppler in the vitreous, which is compatible with vitritis.
- 39. Cataract is an opacification or thickening of the lens and is the leading cause of blindness in the world . Ultrasound Ocular ultrasound is performed when there is suspicion of posterior globe pathology but visualization of the back of the eye is obscured by the opaque lens. Cataract.
- 40. Cataract with retinal detachment.
- 41. Cataract.
- 43. Cataract with retinal detachment.Cataract with uvieitis.
- 44. Annotated ultrasound of an eye with posterior lens luxation. Direct visualization was impossible due to hyphema
- 45. Retinoblastoma is the most common intraocular neoplasm found in childhood, and with modern treatment modalities is, in most cases, curable. Ultrasound Orbital sonography can be performed without sedation and can be repeated multiple times without exposing the child to ionizing radiation. Retinoblastoma's appear as echogenic soft-tissue masses with variable shadowing due to calcifications and heterogeneity due to necrosis and/or hemorrhage. At diagnosis tumours are usually vascular on Doppler examination. The vitreous may have multiple areas of 'floating' debris, which may represent vitreous seeding or alternatively necrotic debris, hemorrhage or increased globulin content.
- 46. RETINOBLASTOMA.
- 47. Retinoblastoma: Large tumor as seen in a 3D ultrasound block demonstrates calcium (arrows).
- 48. Optic disc drusen (ODD) are also known as hyaline bodies and are a relatively common entity. They are usually found incidentally on CT or on follow-up of abnormal fundoscopy. Ultrasound Ocular ultrasound demonstrates an echogenic focus within or on the surface of the optic nerve head. Posterior acoustic shadowing may be present with larger lesions. Fundoscopic findings depend on how deeply the drusen is located in the optic disc. Superficial deposits exhibit characteristic auto fluorescence making the diagnosis in such cases obvious. Deeper deposits have less-specific appearances with swelling of the optic disc that mimics papilloedema (pseudopapilloedema.
- 50. B-scan ultrasound of the right and left eye showing increased reflectivity on the optic nerve head and increased shadowing consistent with optic nerve drusen.
- 51. Staphyloma is the term given to an eye whose sclero-uveal coats are stretched (also known as ectasia). This most commonly occurs posteriorly, although anterior Staphyloma also is recognised. As opposed to coloboma,staphyloma defect is located off-center from the optic disc, typically temporal to the disc Radiographic features increased eye size focal deformity (not as marked as coloboma): usually posterior non-enhancing uveo-sclera. Posterior staphyloma.
- 52. A/B-scan ultrasonography of an eye with posterior staphyloma.
- 53. Hyphema (blood in the anterior chamber). 3.a Eye with hyphema. 3.b: Ultrasound image of the same patient observing the presence of small echogenic areas due to the bleeding (arrow). Hyphema describes the condition of the aqueous humor when red blood cells form a suspension in it.
- 55. Thank You.