Presentation1.pptx, ultrasound examination of the shoulder joint.
•Download as PPTX, PDF•
75 likes•10,671 views


Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (18)
Similar to Presentation1.pptx, ultrasound examination of the shoulder joint.
Similar to Presentation1.pptx, ultrasound examination of the shoulder joint. (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Presentation1.pptx, ultrasound examination of the shoulder joint.
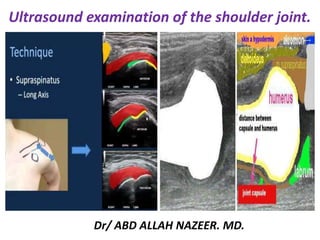
- 1. Ultrasound examination of the shoulder joint. Dr/ ABD ALLAH NAZEER. MD.
- 2. ULTRASOUND OF THE SHOULDER - Normal Transverse Biceps tendon scan plane. Transverse Long Head Biceps.
- 3. Longitudinal Biceps tendon scan plane. Biceps tendon LS normal.
- 4. Subscapularis tendon scan plane. Normal subscapularis.
- 5. Axial view of shoulder anatomy. Coraco-acromial ligament.
- 6. Patient begins with arm by their side and abducts sideways to 90degrees. Look for bunching of bursa or tendon against the acromion or coraco-acromial ligament. Normal supraspinatus LS.
- 7. Normal sub acromial Bursa, The subacromial and subdeltoid bursae are intimately against, and indistinguishable from, the overlying deltoid muscle. The subacromial bursa. The bursae are subject to thickening and /or fluid. This image shows both thickening and fluid. The measurement indicates how little is required to be symptomatic.
- 8. SSP scan plane 2: Patient's hand behind their back. Normal supraspinatus TS.
- 9. ACJ scan plane. AC joint normal.
- 10. Infraspinatus scan plane: Patient's hand towards unaffected shoulder. Infraspinatus.
- 11. Infraspinatus scan plane: Patient's hand towards unaffected shoulder. Abduction: Hover mouse over to see supraspinatus pre and post abduction at the acromion.
- 12. Normal supraspinatus tendon, longitudinal and transverse views.
- 13. Normal Subscapularis tendon-longitudinal and transverse view.
- 14. Normal Infraspinatus tendon-longitudinal view. Acromioclavicular normal joint.
- 15. Tendon of long head of biceps brachii in the bicipital groove longitudinal and transverse view.
- 16. ROLE OF ULTRASOUND Ultrasound is essentially used for the rotator cuff complex of the shoulder. Ultrasound is a valuable diagnostic tool in assessing the following indications; Muscular, tendinous and some ligamentous damage (chronic and acute) Bursitis Joint effusion Vascular pathology Haematomas Soft tissue masses such as ganglia, lipomas Classification of a mass e.g solid, cystic, mixed Post surgical complications e.g abscess, edema Guidance of injection, aspiration or biopsy Some bony pathology. LIMITATIONS It is recognised that ultrasound offers little or no diagnostic information for internal structures such as the gleno-humeral ligaments. Ultrasound is complimentary with other modalities, including plain X-ray, CT, MRI and arthroscopy. EQUIPMENT SELECTION AND TECHNIQUE Use of a high resolution probe (7-15MHZ) is essential when assessing the superficial structures of the shoulder. Careful scanning technique to avoid anisotropy (and possible misdiagnosis) Beam steering or compounding can help to overcome anisotropy in linear structures such as tendons. Good colour / power / Doppler capabilities when assessing vessels or vascularity of a structure. Be prepared to change frequency output of probe (or probes) to adequately assess both superficial and deeper structures.
- 17. Shoulder Ultrasound Technique Lennard Funk, 2008 Indications Indications for ultrasound scanning of the shoulder include: Suspicion of rotator cuff pathology Full thickness cuff tears Partial thickness tears tendonitis/tendinosis Calcific tendonitis Subacromial impingement / bursitis Long Head of Biceps pathology such as tendonitis or tears, subluxation or dislocations. Acromioclavicular Joint pathology such as arthritis, osteolysis and subluxations. Glenohumeral pathologies such as: Glenohumeral arthritis (osteophytes). Glenohumeral effusions. Rarely, labral pathology . Bony lesions such as Hill-Sachs Lesions
- 18. PATIENT POSITION Patient seated on chair in front of ultrasound machine. Have the patient's chair at an appropriate height to be ergonomically comfortable for you to scan. LONG HEAD BICEPS (BT): For example images of pathology, click here to go to the shoulder pathology page. Patient rests hand palm up on thigh. Scan transversely over the anterior humeral head. Visualize the bicipital groove. Identify the biceps tendon in the groove (if not identified it may be either torn or subluxed medially out of the groove). Follow down to the muscle belly. Rotate into longitudinal and re-examine. The tendon should be a uniform fibrillar structure, generally less than 5mm thick. Examine dynamically in a transverse plane during internal/external rotation to ensure it doesn't subluxed medially. SUBSCAPULARIS (SSC): For example images of pathology, click here to goto the shoulder pathology page Again in a transverse plane at the bicipital groove, externally rotate the patient's arm. The SSC tendon will be visible inserting medial to the groove. It will be seen as an elongated slightly convex tendon
- 19. SUPRASPINATUS (SSP) For example images of pathology, click here to goto the shoulder pathology page Position the patient palm up with their elbow flexed and pulled back passed their side so their hand is near their hip. Identify the SSP tendon supero-lateral to the bicipital groove. In a coronal plane, the tendon emerges from beneath the acromion to insert on the greater tuberosity of the humerus. It should be uniform, fibrillar & 'beak shaped' (convex superiorly). INFRASPINATUS (ISP) For example images of pathology, click here to goto the shoulder pathology page Ask the patient to place their affected hand across their chest towards the contralateral shoulder. The ISP can be seen by placing the probe immediately inferior to the spine of the scapula and following the tendon to it's insertion postero-laterally on the humeral head. It will have a similar appearance to subscapularis.
- 20. DYNAMIC ASSESSMENT Biceps: assess it's stability within the bicipital groove during external rotation. Subscapularis: assess for any overlying subdeltoid bursal bunching against coracoid during internal rotation Supraspinatus: assess for bunching of the tendon &/or overlying subacromial bursa against the acromion or coraco-acromial ligament during abduction. Ensure the patient does NOT hunch their shoulder or lean towards the contralateral side during abduction. Posterior joint recess: during internal/external rotation, assess for a gleno-humeral joint effusion. This will be most evident during external rotation Acromio-clavicular joint: During forward flexion with internal rotation look for boney contact or ganglia of the ACJ. A shoulder series should include the following minimum images: Long head biceps tendon - long, trans Subscapularis tendon Coraco-acromial ligament Supraspinatus tendon Infraspinatus tendon Acromio-clavicular joint Posterior joint recess Pre & post abduction views Document the normal anatomy. Any pathology found in 2 planes, including measurements and any vascularity. Detail any limitation to range of movement and degree that pain or symptoms begin.
- 21. Rotator Cuff Injury and Inflammation. Rotator cuff injury and inflammation is one of the most common causes of shoulder pain. There are three common conditions that can affect the rotator cuff: rotator cuff tendonitis, rotator cuff impingement syndrome and a rotator cuff tear. Most people with rotator cuff problems can be successfully treated by a combination of rest, painkillers, anti-inflammatories, physiotherapy and steroid injections. Surgery is sometimes an option. US Imaging.—Sonographic findings for a full-thickness rotator cuff tear include nonvisualization or absence of cuff tissue, a full-thickness hypoechoic defect, focal thinning, loss of the convexity of the outer cuff contour, ability to compress the deltoid muscle within a defect or against the humeral head, visualization of the underlying hyaline cartilage (“naked cartilage sign”) a heterogeneously hypoechoic cuff with bursal fluid, and severe distortion of cuff architecture. In consideration of studies with surgical correlation, reported sensitivities and specificities for US range from 57% to 95% and 76% to 94%, respectively. Not surprising, the sensitivity increases as the size of the tear increases, with sensitivity for massive cuff tears (>3 cm) approaching 100%.
- 22. Sonographic detection, localization, and characterization of partial-thickness cuff tears have been described only recently. Proposed criteria include a hypoechoic defect that involves the articular or bursal surface, a focal hypoechoic zone within the substance of the cuff, a large linear echogenic focus within the cuff substance, thinning of the cuff (marked during passive movement), and a straight outer cuff border (loss of convexity). Criteria that address intrasubstance findings may produce a relatively high false-positive rate because these “defects” may not be visualized by means of correlative methods such as arthrography, arthroscopy, and surgery. Van Holsbeeck et al achieved 93% sensitivity and 94% specificity with two criteria: a mixed hyper- and hypoechoic region or a hypoechoic discontinuity that involves either the bursal or articular surface. The former is attributed to penetration of torn cuff fibers by joint fluid. An associated finding described by these investigators is that of “pitting” of the greater tuberosity
- 23. Full-thickness cuff tear in a 74-year-old woman. A, The longitudinal image shows that the cuff is retracted medially, and the torn tendon end (T) is surrounded by fluid. B, The transverse image shows the width of the tear (between cursors).
- 24. Large, full-thickness tear of the rotator cuff. Coronal (longitudinal) sonogram shows a large cuff defect filled with fluid and debris (straight arrows). Also apparent are the medially retracted edge of the supraspinatus tendon (curved arrow), near apposition of the deltoid muscle (D) to the humeral head, and loss of outer convexity.
- 25. Massive full-thickness tear of the rotator cuff. (a) Coronal (longitudinal) US image demonstrates a massive rotator cuff tear, the gap filled with hypoechoic fluid (straight arrows). The underlying hyaline cartilage is exposed (naked cartilage sign) (curved arrows). (b) Coronal US image obtained with manual compression of the same region of the cuff shows apposition of the deltoid muscle (D) to the underlying humeral head (solid arrows). An osseous excrescence appears at the articular margin (open arrow).
- 26. Full-thickness tear of the rotator cuff. (a) Coronal (longitudinal) US image shows a full- thickness defect of the rotator cuff filled with both fluid and debris (straight arrows). Delamination of the cuff is apparent, with more medial retraction of the deep (solid curved arrow) as opposed to the bursal (open arrow) aspect. In addition, the specular reflector of the articular surface abuts fluid, resulting in the naked cartilage sign (open arrowheads). There is minor osseous irregularity (solid arrowheads).
- 27. Full-thickness tear of the supraspinatus tendon. (a) Longitudinal US image demonstrates a full-thickness hypoechoic defect in the normal location of the supraspinatus tendon (arrows). This defect represents fluid and extends from the bursal surface to the articular surface. Note the torn edge of the retracted supraspinatus tendon (S). (b) Transverse US image shows an intact infraspinatus tendon (i) posterior to the tear. The double cortex sign can also be seen; the overlying fluid accentuates the appearance of the cartilage (arrows), which is almost as hyperechoic as the underlying cortex.
- 28. Full-thickness tear of the rotator cuff.
- 29. Partial-thickness tear of supraspinatus tendon. (A) Short-axis view. There is a partial-thickness articular surface tear in the mid-substance of the tendon (between markers) with a few intact fibers overlying (arrow). (B) Partial-thickness bursal surface tear (arrow) of the supraspinatus tendon. (C) Partial-thickness intrasubstance tear (arrow). (D) Partial tear (rim rent) of supraspinatus tendon at greater tuberosity (arrow). BT: Biceps tendon, HH: Humeral head
- 30. Partial, undersurface tear of the rotator cuff. Coronal (longitudinal) US image shows mixed echogenicity of the undersurface of the cuff (straight arrows) that reflects torn cuff fibers and adjacent fluid. The bursal fibers are intact (curved arrows
- 31. Partial-thickness, undersurface tear of the rotator cuff. Transverse sonogram demonstrates a hypoechoic region (open arrow) along the undersurface of the supraspinatus tendon (SS). The adjacent greater tuberosity is pitted (solid arrows
- 33. Subscapularis tendon tear with subluxation of the long head of the biceps tendon. Transverse US image (a) and axial proton-density–weighted MR image (b) show a tear of the subscapularis tendon (arrow), with the biceps tendon (b) perched on the lesser tuberosity (L).
- 34. Partial tear of the cranial half of subscapularis tendon.
- 35. Tendinosis. On a longitudinal US image, the supraspinatus tendon (arrows) is thickened and heterogeneous with no discrete defects. Instead, an ill- defined hypoechoic defect with indistinct borders is seen (*).
- 36. Marked tendinopathy. The longitudinal image shows a hypoechoic and very thickened cuff.
- 37. Calcific tendinitis. (a) Radiograph demonstrates deposition of calcium hydroxyapatite (arrow) just superior to the greater tuberosity at the insertion site of the supraspinatus tendon. (b) US image shows calcium deposition within the supraspinatus tendon as a lobular echogenic area without shadowing (arrows). Note also the effusion in the subdeltoid bursa (*).
- 38. Supraspinatus tendon calcifying tendonitis.
- 39. Subacromial bursitis is a common cause of shoulder pain that is usually related to shoulder impingement of your bursa between your rotator cuff tendons and bone (acromion). Your subdeltoid bursa is less commonly inflamed shoulder bursa. Ultrasound show fluid distension, synovial proliferation, thickening of the bursal wall. Subacromial- subdeltoid bursal effusion.
- 40. Subdeltoid bursitis. Longitudinal US image of the biceps tendon demonstrates a fluid collection (arrows) superficial to and not involving the biceps tendon (b).
- 42. Shoulder joint effusion tracking into the biceps tendon sheath. Transverse US image (a) and axial gradient-echo MR image (b) demonstrate an effusion in the biceps tendon sheath (arrows). The box in b corresponds to the field of view in a.
- 43. Biceps tendinitis is inflammation of the tendon around the long head of the biceps muscle. Biceps tendinosis is caused by degeneration of the tendon from athletics requiring overhead motion or from the normal aging process. Inflammation of the biceps tendon in the bicipital groove, which is known as primary biceps tendinitis. Biceps tendinitis and tendinosis are commonly accompanied by rotator cuff tears or SLAP (superior labrum anterior to posterior) lesions. Patients with biceps tendinitis or tendinosis usually complain of a deep, throbbing ache in the anterior shoulder. Repetitive overhead motion of the arm initiates or exacerbates the symptoms. Ultrasonography is preferred for visualizing the overall tendon, whereas magnetic resonance imaging or computed tomography arthrography is preferred for visualizing the intraarticular tendon and related pathology. Ultrasound appearance of tendinosis depends on extensity and the time between injury and sonographic evaluation. In acute tendinosis, initially, tendon is thickened, with normal contour and echo structure. As the process progresses, the fibrillar pattern is lost and tendon becomes hypoechoic, with further swelling. Discrete focal hypoechoic areas may represent small partial tears, which may not extend to the tendon surface. But if a defect is present on the tendon surface, dynamic evaluation (i.e., during movement) should be performed to rule out partial tear. Increased Doppler flow can point to hyperemia that can be associated with tendinopathy.
- 45. Biceps brachii tendon tear. Longitudinal scan of the bicipital groove shows proximal retraction of the biceps muscle (long arrow). A fluid-filled gap with echogenic clots (small arrow) at the myotendinous junction.
- 46. Biceps brachii tendon synovitis. Axial scan of the biceps tendon shows fluid and synovial thickening (arrow) surrounding the biceps tendon sheath.
- 47. Biceps tendon subluxation. Transverse scan through the left BG shows an empty groove. Note that the groove in this patient is shallow. The biceps tendon (arrow) lies medially, anterior to the lesser tuberosity of the humerus. A small amount of fluid is seen in the tendon sheath.
- 48. Degeneration of the tendon of long head of biceps brachii-transverse view.
- 58. Recurrent Rt. shoulder anterior dislocation (fibrous Bankert lesion with Hill-Sachs deformity). (Real-time U/S., T.S.) of the Rt. Shoulder at the level supraspinatus tendon revealed; triangular bony depression (arrowed) in the postero superolateral aspect of the humeral head with its base toward cutaneous surface (hill-Sachs lesion).
- 71. Synovial chondromatosis is a benign condition characterized by synovial proliferation and metaplasia, with development of cartilaginous or osteocartilaginous nodules within a joint, bursa or tendon sheath. In the shoulder, synovial osteochondromatosis may occur within the glenohumeral joint and its recesses (including the tendon sheath of the biceps long head), and in the subacromial-deltoid bursa. Such condition can be identified either by radiography, ultrasonography or magnetic resonance imaging, showing typical features according to each method. Radiography commonly shows ring-shaped calcified cartilages and periarticular soft tissues swelling with erosion of joint margins. Ultrasonography demonstrates hypoechogenic cartilaginous nodules with progressive increase in echogenicity as they become calcified, with development of posterior acoustic shadow in case of ossification. Besides identifying cartilaginous nodules, magnetic resonance imaging can also demonstrate the degree of synovial proliferation.
- 72. Secondary synovial osteochondromatosis. Sonographic study of the shoulder focusing the tendon of the biceps long head (TBLH) on the transverse plane. Presence of synovial nodules with different levels of echogenicity projecting toward the interior of the tendinous sheath, easily identifiable by the presence of synovial fluid. The echogenicity depends on the calcification degree, with hypoechoic nodules (black arrow) corresponding to noncalcified chondromas, while calcified nodules present increased echogenicity (arrowhead).
- 73. Secondary osteochondromatosis. Sonographic study of the shoulder, focusing the tendon sheath of the biceps long head on the longitudinal plane. The sheath is filled by fluid, and in its interior calcified nodules with posterior acoustic shadow are identified (arrows).
- 74. Secondary synovial osteochondromatosis associated with supraspinatus tendinopathy. A: Sonographic study of the shoulder focusing the tendon of the biceps long head on the longitudinal plane, which is ruptured, with only its proximal stump being identified. Multiple small synovial chondromas and effusion within the synovial sheath are observed. B: Longitudinal section of the supraspinatus tendon. Thickened, hypoechoic and heterogeneous tendon, with loss of fibrillar structure, characterizing tendinopathy process.
- 75. Thank You.