Presentation1.pptx, ultrasound examination of the wrist joint.
•Download as PPTX, PDF•
66 likes•12,302 views


Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Presentation1.pptx, ultrasound examination of the wrist joint.
Similar to Presentation1.pptx, ultrasound examination of the wrist joint. (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Presentation1.pptx, ultrasound examination of the wrist joint.
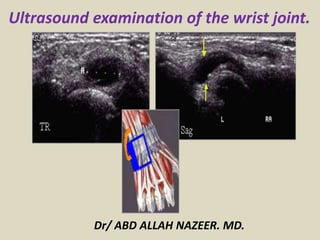
- 1. Ultrasound examination of the wrist joint. Dr/ ABD ALLAH NAZEER. MD.
- 2. ULTRASOUND OF THE WRIST – Normal. Dorsal Wrist Compartments.
- 3. Compartment 1 scan plane:
- 4. Compartment 2 Scan plane: Extensor Carpi Radialis, Longus and Brevis. Transverse view of the extensor carpi radialis longus and brevis tendons.
- 5. Scapho lunate ligament scan plane Scapho-lunate ligament is seen as a fibrillar tight band. Visualizing the SCL does not exclude carpal instability.
- 6. Compartment 3 scan plane: Extensor Pollicis Longus. The EPL tendon is tucked against Lister's Tubercle. The Extensor digitorum longus common tendon is adjacent in compartment 4.
- 7. Compartment 4 Scan plane: Extensor digitorum. The common extensor digitorum tendon divides into 4 prior to the wrist crease.
- 8. Common extensor Digitorum with the overlying extensor retinaculum. Compartment 5: Extensor digiti minimi, immediately medial to the extensor digitorums.
- 9. Compartment 6 Scan plane: Extensor Carpi Ulnaris. Extensor carpi ulnaris.
- 10. ANTERIOR WRIST. A basic schematic of the anterior wrist tendons and Carpal Tunnel.
- 11. Scan plane for the carpal tunnel. Transverse carpal tunnel. Flexor carpi radialis (FCR); Flexor Pollicis Longus (FPL); Median Nerve (MN); Flexor Digitorums.
- 12. Scan plane for the FCR tendon. The flexor carpi radialis tendon curving over the scaphoid to insert onto the 1-2 metacarpal bases.
- 13. Scan plane for the FCU tendon. The Flexor Carpi Ulnaris tendon
- 18. Indication for wrist ultrasound study.
- 19. ROLE OF ULTRASOUND Ultrasound is a valuable diagnostic tool in assessing the following indications in the wrist: Muscular, tendinous and ligamentous damage (chronic and acute) Bursitis Joint effusion Vascular pathology Haematomas Soft tissue masses such as ganglia, lipomas Classification of a mass e.g solid, cystic, mixed Post surgical complications e.g abscess, edema Guidance of injection, aspiration or biopsy Relationship of normal anatomy and pathology to each other Some bony pathology.
- 20. LIMITATIONS Recent surgery or injections may degrade image quality through the presence of air in the tissue. EQUIPMENT SELECTION Use of a high resolution probe (10-15MHZ) is essential when assessing the superficial structures of the wrist. Careful scanning technique to avoid anisotropy (and possible misdiagnosis). Beam steering or compounding can help to overcome anisotropy in linear structures such as tendons. Good colour / power / Doppler capabilities when assessing vessels or vascularity of a structure. Be prepared to change frequency output of probe (or probes) to adequately assess both superficial and deeper structures.
- 21. The posterior wrist is conveniently divided into 6 compartments: Abductor pollicis longus(APL) and Extensor Pollicis Brevis (EPB) Extensor Carpi Radialis (ECR) longus and Brevis Extensor Pollicis Longus (EPL) Extensor Digitorum (ED) Extensor Digiti Minimi (EDM) Extensor Carpi Ulnaris (ECU) These are all tethered by the extensor retinaculum which overlies ,and in some areas reflects around, the tendons. Begin by scanning over the lateral wrist crease at the anatomical "snuff-box". You should see the APL & EPB in compartment 1. To check, both tendons should be able to be followed up the thumb. If they go to the carpus you have slipped medially onto compartment 2. Work your way sequentially across the wrist assessing each tendon individually. De Quervain,s tenosynovitis Inflammation of the Abductor Pollicis Longus and Extensor pollicis Brevis tendons. Overuse injury. Patients present with focal, point tenderness laterally over the radial styloid.
- 22. Proximal intersection syndrome Extensor Pollicis Brevis crossing over extensor Carpi Radialis longus & Brevis. Distal intersection syndrome Ext Pollicis Longus crossing over extensor Carpi Radialis longus & Brevis. Scapho-lunate ligament The wrist is essentially divided into 3 joint planes: 1. and 2. The radiocarpal and midcarpal Joints allow wrist flexion, extension and lateral deviation. 3. The distal radio-ulnar joint allows the forearm and hand to rotate. (Pronation / Supination). These joints are supported by a series of extrinsic and intrinsic ligaments. The scapholunate ligament is the most important dorsal intrinsic stabilizer. Injury occurs with a hyperextension of the wrist. Similar mechanism to a scaphoid fracture but results in a ligament tear instead. If only a partial tear it is usually stable. If complete, it results in Scapho-lunate instability. The scaphoid will rotate abnormally during wrist movement, which if left untreated can lead to significant chronic wrist degeneration.
- 23. ANTERIOR WRIST:
- 24. Carpal Tunnel Syndrome This is the most common peripheral nerve entrapment. It occurs when the median nerve is compressed by the overlying flexor retinaculum. IMPORTANT: Ultrasound cannot exclude Carpal tunnel syndrome. The accepted standard for diagnosis is a nerve conduction study. Our role is to identify possible causes for the patient's symptoms. Look for: Tendon abnormalities Ganglia Fluid Accessory muscles Any asymmetry with the contra lateral side. There have been several proposed methods of quantitative assessment for carpal tunnel. In our experience, these have not been reliable. They include: Nerve cross sectional area of >10square mm proximal to the retinaculum. Nerve flattening ratio of 3:1.
- 25. Guyons Canal Syndrome Canal bordered by the pisiform & hamate and roofed by a reflection of the flexor retinaculum. The ulna nerve and artery pass through and may become entrapped or injured. Repetitive injury such as cycling or using heel of hand as hammer. On Ultrasound: As with carpal tunnel look for ganglia, accessory muscles and asymmetry with the contra lateral side Triangular Fibro-Cartilage Complex (TFCC) A section of cartilage and ligaments at the distal ulna. Provides a continuous gliding surface along the forearm- carpal joint. Affected by: Natural degeneration with age.
- 26. Detection of Effusion in the volar recess of the PIP joint – longitudinal and transverse views. A joint effusion is defined as an increased amount of fluid within the synovial compartment of a joint. There is normally only a small physiological amount of fluid. Abnormal fluid accumulation can result from inflammation, infection (i.e. pus) or trauma and may be an exudate, transudate, blood and/or fat.
- 27. Effusion noted on longitudinal view over the radiocarpal joint.
- 28. TFCC tears can be degenerative and occur after the third decade. They are usually asymptomatic and have to be differentiated from traumatic tears. Palmer’s classification aims to classifying the kind and location of tear. Central tears (type IA) are common and are located at the horizontal portion of the articular disk just 2 to 3 mm from the radial origin. Ulnar tears (type IB) are less common but may lead to DRUJ instability if they are not diagnosed at an early stage. Recent studies have described new entities such as ‘bucket-handle’ tears or association between different types of tears. Ultrasound allows a partial visualization of the TFCC because the size of the acoustic window varies with the size and the morphology of the ulnar styloid and the ulnar variance. Articular disk assessment may be limited if there is a positive ulnar variance or if the ulnar styloid is hypertrophic. According to recent studies, sensitivity ranged from 63 to 100% whereas specificity was 100%. Nevertheless, it is not possible to distinguish degenerative tears from traumatic ones and the location of tears has not been described in those studies. For these reasons, ultrasound is not the modality of choice in order to assess TFCC integrity. CT may show indirect sign of TFCC injuries if DRUJ dislocation is present.
- 29. Central and peripheral TFC disk tears. Coronal T1W MRA image of the wrist with fat suppression (A) and longitudinal sonoarthrogram of the TFC disk (B) in the same patient show a central TFC disk tear (arrow). Note the leak of radiocarpal joint contrast into the distal radioulnar joint in A and the leak of radiocarpal joint contrast through the ulnar joint capsule into the adjacent soft tissues through the peripheral TFC complex tear in A and B (arrowheads).
- 30. Triangular fibrocartilage disk tear. On all images, the distal ulna is on the left, and the triquetrum is on the right. A, Longitudinal sonogram shows a hypoechoic appearance of the central aspect of the TFC disk, consistent with a tear (arrows). B, Longitudinal sonogram in a different patient shows an area of abnormal hypoechogenicity at the periphery of the TFC disk (arrow) under the ECU, consistent with a peripheral tear. C, Longitudinal sonoarthrogram in the same patient as in B improves visualization of the peripheral TFC disk tear and shows extension of intra-articular contrast in an additional TFC disk cleft/tear (arrow).
- 31. Ganglion cysts are non-malignant cystic masses that occur in association with musculoskeletal structures. They are sometimes also simply referred to as ganglia or a ganglion, but should not be confused with the anatomical term ganglion. Ultrasound The vast majority are anechoic to hypoechoic on ultrasound and have well defined margins. Many demonstrate internal septations as well as acoustic enhancement. Dorsal Ganglion cyst.
- 32. Wrist Ganglion
- 33. Wrist Ganglion
- 34. Ultrasound in axial plane shows torn (a) and normal fibrillar appearance (b) of the scapholunate ligament. SCAPHOLUNATE LIGAMENT TEARS The scapholunate (SL) ligament is an intrinsic ligament between the scaphoid and lunate with three bundles: Dorsal and ventral bundles are composed of collagen fibers. The dorsal one is thicker and plays a major role in wrist stability. Central (or proximal) bundle is fibrocartilaginous and may present degenerative and asymptomatic changes in elderly patients. Ultrasound is a widely available technique and is useful to assess the SL ligament. The visibility of the ligament varies from 91 to 98% due to its superficial location. The dorsal segment is superficial and can be easily assessed just distally to the Lister’s tubercle.
- 42. Carpal tunnel syndrome (CTS) is results from compression of the median nerve within the carpal tunnel. It is a cause of significant disability, and is one of three common median nerve entrapment syndromes; the other two being anterior interosseous nerve syndrome and pronator teres syndrome. Ultrasound In imaging median nerve syndromes, ultrasound is useful in examining CTS, potentially revealing, in fully developed cases, a triad of: palmar bowing of the flexor retinaculum (>2 mm beyond a line connecting the pisiform and the scaphoid) distal flattening of the nerve enlargement of the nerve proximal to the flexor retinaculum Enlargement of the nerve seems to be the most sensitive and specific criterion, but what cut-off value for pathological size remains debated; normal cross-sectional area is given at 9-11 mm, but the range of sizes deemed pathological is wide. One study has calculated that a 2 mm difference in nerve cross-section between the level of the pronator quadratus and the carpal tunnel has a 99% sensitivity and 100% specificity for CTS
- 43. Carpal tunnel syndrome with thickened median nerve.
- 44. Carpal tunnel syndrome in bifid median nerve.
- 45. Carpal tunnel syndrome with inverted notch sign.
- 46. A 36-year-old male with symptoms of CTS. Transverse USG shows scar tissue (arrow) at the site of decompression.
- 47. CTS. Longitudinal USG shows proximal synovial bulge (arrow) with hypoechoic exudative tenosynovitis.
- 48. CTS. Transverse USG shows scar tissue at the site of surgery (arrow) and incomplete division of the flexor retinaculum (arrowheads).
- 49. Carpal tunnel syndrome. Transverse sonogram showing reformed flexor retinaculum (pink arrow) and flattened median nerve (blue arrow)
- 50. CTS. Transverse USG shows reformed flexor retinaculum (arrow), median nerve (arrow head), and the muscle belly of the flexor digitorum profundus (star)
- 51. Carpal tunnel syndrome. Transverse sonogram showing neurogenic tumor at the carpal tunnel.
- 52. Guyon's Canal Syndrome: Your wrist has "tunnels" or "canals" through which some nerves and blood vessels pass. Guyon's canal is located along the lower edge of your palm, on the little finger side of your hand. Your ulnar nerve and artery run through this canal, where the nerve splits into two terminal branches that go on into your palm, ring and little fingers. Compression or entrapment of the ulnar nerve at the canal leads to pain, tingling and numbness in the left side of your palm and in your ring and little fingers. CAUSES : The disorder is caused by pressure on the ulnar nerve. This is most likely the result of external pressures (handlebars on a bike), but may also be internal (tumor, cyst, fracture or aneurysm of the ulnar nerve). RISK INCREASES WITH: Diabetes mellitus. Underactive thyroid gland (hypothyroidism). Menopause. Raynaud's disease (vascular disorder). Long-distance cycling. Repeated jolting or shaking of the hands or wrist. Gout. Sports that may cause fracture of the hamate bone in the hand (baseball batting, golf, tennis, badminton). Rheumatoid arthritis. Ganglion cyst. Carpal tunnel syndrome.
- 54. Guyon's Canal Syndrome secondary to space occupying lesion.
- 55. Ulnar nerve irritation at the Guyons canal.
- 56. Tenosynovitis is a term describing the inflammation of the synovial membrane surrounding a tendon. The synovial membrane is part of a fluid- filled sheath that surrounds a tendon Etiology Tenosynovitis can be caused by a variety of disease processes, including, but not limited to: injury rheumatic disease infection mechanical irritation compartment syndrome gout pseudo gout / CPPD diabetes Ultrasound On ultrasound, the synovial membrane is not identified unless there is pathological swelling. We can find increased fluid content within tendon sheath, a thickening of the synovial sheath, peritendinous subcutaneous edema resulting in a hypoechoic halo sign and peritendinous subcutaneous hyperemia on Doppler imaging.
- 63. Active synovitis overlying a large metacarpal head erosion.
- 64. Longitudinal view of the wrist revealing active synovitis
- 65. Crystalline arthropathy. Longitudinal and transverse views of the first MTP revealing tophaceous dorsal deposit as well as double contour sign.
- 67. Acute tenosynovitis of common extensor tendon of wrist.
- 68. Acute inflammation of common extensor tendon of hand. Transverse image showed thickening and decrease the echogenicity (arrows) in the tendon sheath, with hypervascularity in CDUS. This is acute tenosynovitis case. MC: metacarpal bones.
- 69. Tenosynovitis of 6th compartment (extensor carpi ulnaris tendon) (arrows). US image showed thickening of tendon sheath (arrows)
- 70. Septic arthritis and tuberculous arthropathy is one of the common cause of infectious arthritis is developing countries. Any pathological joint lesion where the exact diagnosis is equivocal, should be considered tubercular in origin unless proven otherwise. Risk factors for septic arthritis include bacteraemia, advanced age, an immunocompromised state, rheumatoid arthritis, intraarticular injections, and prosthetic joints Ultrasound Joint effusion may be the only finding but is non- specific.
- 71. Hand and wrist abscesses.
- 72. TB granuloma. 2: 2nd metacarpal bone, 3: 3rd metacarpal bone.
- 73. De Quervain tenosynovitis, also known as washerwoman's sprain/strain, is a painful stenosing tenosynovitis involving the first extensor (dorsal) tendon compartment of the wrist (typically at the radial styloid). This compartment contains the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) tendons. Ultrasound Ultrasound is very often diagnostic. Findings include: oedematous tendon thickening of APL and EPB at level of radial styloid (compare with contralateral side) increased fluid within the first extensor tendon compartment tendon sheath thickening of overlying retinaculum and the synovial sheath peritendinous subcutaneous edema resulting in a hypoechoic halo sign peritendinous subcutaneous hyperemia on Doppler imaging It is important to assess for an intratendinous septum which can usually be identified if present. Ultrasound is often used to guide corticosteroid injections into the tendon compartment to treat the condition.
- 74. De Quervain,s syndrome. Transverse section of APL and EPB tendons showed thickening tendon sheath over EPB tendon, and CDUS showed hypervascularity. Tenosynovitis of EPB is considered. APL: abductor pollicis longus tendon, EPB: extensor pollicis brevis tendon
- 75. De Quervain’s tenosynovitis: Transverse section of APL and EPB tendons showed thickening tendon sheath (arrows) over the common tendon of EPB and APL. CDUS showed hypervascularity. APL: abductor pollicis longus tendon, EPB: extensor pollicis brevis tendon
- 77. Foreign body
- 78. Giant cell tumours of the tendon sheath (GCTTS) is an uncommon and usually benign lesion that arises from the tendon sheath. It is unclear whether these lesions represent neoplasms or simply reactive masses . It is also known as pigmented villonodular tumour of the tendon sheath (PVNTS) or extra-articular pigmented villonodular tumor of the tendon sheath. Ultrasound Ultrasound is useful as it allows not only characterization of the lesion but also is able to demonstrate the relationship with the adjacent tendon. On dynamic scan, there is free movement of the tendon within the lesion. These masses are typically homogeneously hypoechoic, although some heterogeneity may be seen in echo-texture in a minority of cases . Most will have some internal vascularity.
- 79. Giant cell tumor of wrist.
- 80. Giant cell tumor of metacarpal.
- 81. Thank You.