
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Sarcoidosis
Similar to Sarcoidosis (20)
More from akifab93
More from akifab93 (20)
Recently uploaded
Recently uploaded (20)
Sarcoidosis
- 2. Introduction Non – caseating granulomatous inflammatory disease Most common involvement - Lungs 2 or more organs should be involved for specific diagnosis Womens > Mens Bimodal : 3rd decade and 6th decade 5% have a family history of sarcoidosi.
- 3. Etiology Unknown Few infective and non infective causes has been known MC Infection - Propionibacterium acne > Mycobacterium
- 4. Inclusion body seen in Giant cell in sarcoidosis S - Schaumann bodies A - Asteroid bodies R - Residual bodies C O I D O S I S
- 5. Pathophysiology T-Cells are the most important in pathogenesis . (T-Helper – CD4) HLA-DRB1 is involved in 95% patient - Good prognosis. Macrophages are also involved. Antigen presenting cell (APC) binds toT-cell and activates it. T-cell releases IL-2 and macrophage releasesTNF and IFN-¥. Thus HIV patients with low CD4 count rarely develops Sarcoidosis. Granulomas resolves in most of the patient on its own. But in 20% patient chronicity is seen. IL-8 is responsible for chronic changes.
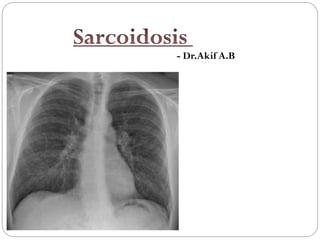
- 7. Lung in sarcoidosis MC involved >90% Infiltrates primarily involves upper lobe. 50% patients presents with obstructive symptoms due to external compression. Rest presents as ILD Staging Stage 1 Hilar adenopathy alone Stage 2 Hilar adenopathy with pulmonary infiltrates Stage 3 Pulmonary infiltrates Stage 4 fibrosis
- 8. Skin in Sarcoidosis Erythema nodosum Lupus pernio - 2nd most commonly invoved - Skin (25%)
- 9. Other organ involved Eye - Anterior Uveitis Liver - Elevated Alkaline phophatase (Cholestatic pattern) Hematologial - Lymphopenia (due to sequestration at inflammation site) Cardiac - Arrhythmias and CHF Hypercalcaemia - Due to increased production of 1,25(OH)Vit.D Renal nephropathy is due to hypercalcaemia. Myalgias and arthralgias Breast lesion Cranial nerve - 7th (Bell’s [Palsy)
- 10. Causes of B/L Hilar adenopathy TB Malignancy Silicosis or beryliosis Extrinsic allergic alveolitis Sarcoidosis
- 11. Investigations Lymphopenia Chest Xray Gallium scan : PET has replaced it now : Increase activity in parotid and Lacrimal gland (PANDA sign) or right paratracheal or Left Hilar area (LAMBDA Sign) Hilar lymphadenopathy >2cm in short axis is more in favour of Sarcoidosis. PET Scan : to look for other granulomatous areas BAL : Lymphocytosis or CD4/CD8 >3.5 PANDA Sign
- 13. Serum ACE Elevated in 60% of acute patients 20% of chronic patients Patients on ACE Inhibitors will have falsely low values False positive : Gaucher’s disease Hyperthyroidism MiliaryTB Leprosy Silicosis,Asbestosis, Beryliosis TB Diabetes : But rise is <50% of normal
- 15. Kveim Siltzbar Procedure Specific diagnostic test Tissue of the spleen of sarcoid patient is taken Injected intradermally in patient with suspect of Sarcoidosis Skin Biopsied after 4-6weeks If shows non caseating granuloma – confirm sarcoidosis Test is obsolete now due to lack of tissue
- 18. Prognosis Many patients resolves within 2-5yr (>95%) Patients requiring steroids in first 6months of presentation are more prone to have chronicity