
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Wiring Tibial Tubercle Fractures
Similar to Wiring Tibial Tubercle Fractures (20)
More from Arun Shanbhag
More from Arun Shanbhag (12)
Recently uploaded
Recently uploaded (20)
Wiring Tibial Tubercle Fractures
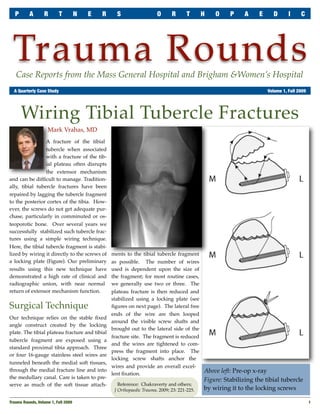
- 1. P A R T N E R S O R T H O P A E D I C Trauma Rounds Case Reports from the Mass General Hospital and Brigham &Women’s Hospital A Quarterly Case Study Volume 1, Fall 2009 Wiring Tibial Tubercle Fractures Mark Vrahas, MD A fracture of the tibial tubercle when associated with a fracture of the tib- ial plateau often disrupts the extensor mechanism and can be difficult to manage. Tradition- ally, tibial tubercle fractures have been repaired by lagging the tubercle fragment to the posterior cortex of the tibia. How- ever, the screws do not get adequate pur- chase, particularly in comminuted or os- teoporotic bone. Over several years we successfully stabilized such tubercle frac- tures using a simple wiring technique. Here, the tibial tubercle fragment is stabi- lized by wiring it directly to the screws of ments to the tibial tubercle fragment a locking plate (Figure). Our preliminary as possible. The number of wires results using this new technique have used is dependent upon the size of demonstrated a high rate of clinical and the fragment; for most routine cases, radiographic union, with near normal we generally use two or three. The return of extensor mechanism function. plateau fracture is then reduced and stabilized using a locking plate (see Surgical Technique figures on next page). The lateral free ends of the wire are then looped Our technique relies on the stable fixed around the visible screw shafts and angle construct created by the locking brought out to the lateral side of the plate. The tibial plateau fracture and tibial fracture site. The fragment is reduced tubercle fragment are exposed using a and the wires are tightened to com- standard proximal tibia approach. Three press the fragment into place. The or four 16-gauge stainless steel wires are locking screw shafts anchor the tunneled beneath the medial soft tissues, wires and provide an overall excel- through the medial fracture line and into Above left: Pre-op x-ray lent fixation. the medullary canal. Care is taken to pre- Figure: Stabilizing the tibial tubercle serve as much of the soft tissue attach- Reference: Chakraverty and others; J Orthopaedic Trauma, 2009; 23: 221-225. by wiring it to the locking screws Trauma Rounds, Volume 1, Fall 2009 1
- 2. P A R T N E R S O R T H O P A E D I C T R A U M A R O U N D S Post-operative Care Patients are maintained at touch down weight bearing in a range of motion brace for six weeks to protect the plateau, but are allowed full, active, and passive range of motion from day one. Key Learning Points Use a proximal tibia locking plate for this kind of operation. Whether the cerclage wires used to tie down the tubercle are placed before or after the locking plate is not important. The critical factor is that the wires pass around locking screws. Right top: Wires are tunneled and passed around screw shafts Right below: Fragment is reduced into place by tightening the wires Far right: Post-operative x-ray Trauma Faculty Mark Vrahas, MD — 617-726-2943 Dear Co!eague: Partners Chief of Orthopaedic Trauma mvrahas@partners.org Thank you for taking the time to read the first edition of Partners Orthopaedic Mitchel B Harris, MD — 617-732-5385 Trauma Rounds. We hope these Rounds provide you with useful information that Chief, BWH Orthopedic Trauma you can apply to your practice. mbharris@partners.org R Malcolm Smith, MD, FRCS — 617-726-2794 We plan to publish quarterly both on paper and on our website: Chief, MGH Orthopaedic Trauma http://achesandjoints.org/Trauma. Each issue wi! feature an article authored by rmsmith1@partners.org one of our Partners Orthopaedic Trauma faculty, whom you wi! be able to con- David Lhowe, MD — 617-724-2800 tact directly with your questions and feedback. MGH Orthopaedic Trauma dlhowe@partners.org The Partners Orthopaedic Trauma Service is a combined clinical and academic David Ring, MD — 617-724-3953 entity which spans the campuses of the Massachusetts General Hospital and MGH Hand & Upper Extremity Service dring@partners.org Brigham & Women’s Hospital. This year, we celebrate our Tenth Anniversary. George Dyer, MD — 617-732-6607 We could not have come this far without your support – our partners in the com- BWH Hand & Upper Extremity Service munity. gdyer@partners.org In this new venture, we welcome your comments and su'estions for future topics. Program Director Suzanne Morrison, MPH Best regards, (617) 525-8876 smmorrison@partners.org Please send correspondence to: Trauma Rounds Editor in Chief Editor, Publisher Yawkey Center for Outpatient Care, Suite 3C Mark Vrahas, MD Arun Shanbhag, PhD, MBA 55 Fruit Street, Boston, MA 02114 2 Trauma Rounds, Volume 1, Fall 2009