2. Introduction:
Developmental
aberration of a tooth resulting in
formation of an accessory cusp
Abnormal
tubercle, elevation,
excrescence, extrusion, or bulge.
Enamel
protuberance,
covering a dentinal core that usually
contains pulp tissue that on occasion may have a
slender pulp horn which extends various distances
up to the full length of the tubercle’s dentin core.
3. The
presence of pulp within the cusp-like
tubercle has great clinical significance and
distinguishes the anomaly from supplemental
cusps, such as the cusp of Carabelli.
Asian
descent (including Chinese, Malay, Thai,
Japanese, Filipino, and Indian populations)
with varying estimates reported at 0.5 to 4.3%
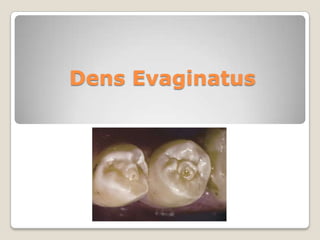
4. Most commonly seen on lingual surface of anterior
teeth (mainly maxillary lateral incisors) & Occlusal
surface of mandibular premolars.
There is typically a bilateral, symmetric distribution,
with a slight sexual predilection for females.
5. Etiology :
Remains
undetermined.
Autosomal
dominant
and
X-linked
dominant inheritance patterns are seen,
Localized
trauma, possibly from pressure
exerted upon the developing tooth bud
has been suggested.
6. Synonyms
Odontome,
odontoma (odontome) of the axial core
type, evaginatus odontoma (evaginated odontome)
Occlusal
enamel pearl, occlusal tubercle, tuberculum
anomalous,
Accessory
cusp, supernumerary cusp, interstitial
cusp, tuberculated cusp,
Tuberculated
cusp
premolar, Leong’s premolar, and talon
7. Pathophysiology:
An abnormal proliferation and folding of a
portion of the inner enamel epithelium
and subjacent ectomesenchymal cells of
the dental papilla
Into the stellate reticulum of the enamel
organ
During the bell stage of tooth formation
9. Malocclusion with the opposing tooth upon
the cusp-like elevation occurs as involved
teeth erupt into the dental arches.
The resultant occlusal traumatic force
causes abnormal wear or fracture of the
tubercle,
and is the usual manner of pulp exposure
for this anomaly
10.
11.
12. A 20 year old female was referred for
consult and treatment of mandibular right
posterior tooth. Patient was concerned
about the ‘bubble on her gums’.
Occlusal tubercle present in all four
mandibular premolars & an associated
Periapical radiolucency w.r.t. 44
13.
EPT: Except #44 other
teeth were vital.
Root canal therapy of
#44.
Reduction
of
opposing tooth contact
and
composite
restoration of #34, 35,
45.
14.
Calcium hydroxide
root canal dressing
was performed 15
days for the period
of four months.
Obturation of the
tooth was done
using gutta-percha
and
endodontic
sealer (Endoflas FS)
16. References
1.
2.
3.
4.
5.
6.
Marc E. Levitan, Van T. Himel Dens Evaginatus: Literature Review,
Pathophysiology, and Comprehensive Treatment Regimen . J
Endod 2006;32:1–9
Neville B, Damm D, Allen C, Bouquot J. Oral and maxillofacial
pathology, 2nd ed. Philadelphia: WB Saunders, 2002;77–9.
Ash M. Wheeler’s dental anatomy, physiology and occlusion, 8th
ed. Philadelphia:WB Saunders, 2003;241–2.
Kocsis G, Marcsik A, Kokai E, Kocsis K. Supernumerary occlusal
cusps on permanent human teeth. Acta Biol Szeged 2002;46:71–
82
Stewart R, Dixon G, Graber R. Dens evaginatus (tuberculated
cusps): genetic and treatment considerations. Oral Surg Oral Med
Oral Pathol 1978;46:831– 6.
Davies P, Brook A. The presentation of talon cusp: diagnosis,
clinical features, associations and possible aetiology. Br Dent J
1985;159:84–8.