2. ABSTRACT
One of the most interesting congenital malformations is
a conjoined twin. Conjoined twins are a rare
occurrence. More commonly known as Siamese
twins,after First Siamese twins "exhibited" in America in
1829 ,Chang and Eng born in SIAM(Thailand)
•Current technology is providing a basis for earlier
diagnosis and a better prognosis.Magnetic resonance
imaging and CT scan provide excellent anatomic detail,
demonstrating organ position, shared viscera, and
vascular anatomy.
•We present a case of Thoraco-omphalopagus
Conjoined Twins.
3. Case report
22 year old women, primigravida,with 7 months of amenorrhea , 2nd degree
consanguineous marriage & no family history of twins. She had a previous antenatal
Ultrasound report at 16weeks which read as twin pregnancy. She presented to our
hospital at 31 weeks. Sonography was performed which showed following:
•Two fetuses with all 4 pair of limbs and two cranial cavities(dicephalus, tetrabrachius)
•The twins were joined at the thorax and upper abdomen.
•Single umbilical cord(5vessel), shared liver,omphalocoele, and only one fetal heart which
appeared normal.
•One fetus (acardia)had hydrocephalus with poor visualization of lungs and kyphoscoliotic
spine.
•To confirm our findings and get more details we did a fetal MRI.MRI confirmed our usg
findings.
•On the basis of these findings, the diagnosis of terata anacatadidyma, thoracoomphalopagus, conjoined twins was made, and the parents were informed about the
malformation and the twins' poor chance for survival. The parents decided to terminate
the pregnancy.Caesarean section was done and twins were delivered as breech.
•Twins had single male external genitalia, weighing 3 kg together. Placenta was single.
• An USG and CT w was done to further assess them; findings of antenatal scans were
confirmed.
9. INTRODUCTION
• Conjoined twins are rare, but the exact
prevalence is unknown. The estimated
prevalence in the literature varies widely from
1: 50,000 to 1: 200,000.
• There is a female predominance on the order
of 3:1
• The conjoined twinning process occurs when
the division of the embryonic disc occurs more
than 14 days after fertilization.
10. EMBRYOLOGY
• The twinning process occurs in the very early stages of
embryogenesis. Division after the 14th day of fertilization
results in an incomplete division, because once it becomes an
embryo, it is incapable of fusion. The later the division, the
more severe the effect.
• Duplicata incompleta is the most severe form of incomplete
division, because division is so late and incomplete, only a few
organ systems are duplicated. This makes surgical division
impossible.
• Many variations of conjoined twins are possible. It is
customary to name these large lateral fusions, which
incorporate multiple regions, on the basis of the anatomic
part that remains double and separate; for example,
dicephalus, two heads with fusion of the thorax and abdomen
11. •
•
•
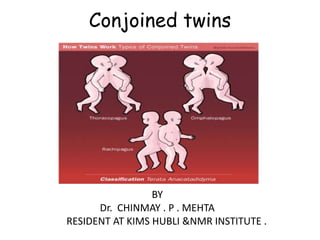
CLASSIFICATION
Inferior conjunction: lower body is single, or twin joined by some lower portion of
.
the body
Duplicata completa = terata catadidyma
Ischiopagus: joined by the lower portion of the coccyx & sacrum
Pygopagus: joined by the lateral and posterior aspect of the coccyx and sacrum
Middle conjunction: midbody fusion with separation of the upper and lower
portion of the body
• Duplicata completa = terata anacatadidyma
Thoracopagus: joined by the chest wall
Omphalopagus: joined between the umbilicus and the xyphoid process
Rachipagus: joined by the spine, above the sacrum
• Superior conjunction: upper body is single, or twin joined by some lower portion
of the body
• Duplicata completa = terata anadidyma
Syncephalus: joined by the face
Craniopagus: joined by the skull.
( Site of fusion + suffix "pagus“)
12.
13. USG DIAGNOSIS CRITERIA
• Demonstration of a continuous non seperated external skin
contour.
• Bifid appearance of the fetal pole in first trimester
• Conjoined body parts.
• Body parts of the twins are imaged on the same level and
in the same sonar plane.
• No change in the relative position of the twins to one
another and on successive scans.
• Monochorionic twinning-Single placental mass/ No intertwin membrane
• More than 3 vessels in a single umbilical cord.
• Complex multiple fetal anomalies.
14. THORACOPAGUS
• Thoracopagus twins are united face to face from the upper
thorax to the umbilicus with a common sternum, diaphragm,
and upper abdominal wall. Ninety percent of such twins have
a common pericardial sac, and there is always a degree of
cardiac fusion.
• The liver is invariably fused, and 25% of thoracopagus twins
share a biliary system. Initial liver assessment can be
performed with US. However, in twins joined anteriorly, there
is limited probe access; when viewed from the side, the
conjoined liver is oriented in an oblique plane to the axis of
the probe .
• A better appreciation of liver anatomy is gained from
multiplanar techniques, ideally MR imaging.
• It is important to evaluate bile excretion by using dynamic
biliary scintigraphy with Tc-99m HIDA
15. OMPHALOPAGUS
• Omphalopagus twins are joined ventrally in the
umbilical region, often including the lower
thorax.
• Liver fusion occurs in approximately 80% of cases.
As there is no mixing of blood in the cardiac
chambers, the liver can be well assessed by using
CT with intravenous injection of contrast material
into one twin.
• Gadolinium-enhanced MR imaging can also be
used in this context. As described in the section
on thoracopagus twins, biliary scintigraphy can be
helpful in determining biliary drainage
16. ROLE OF COLOR DOPPLER & 4D
• Color doppler is very useful in evaluation of
liver blood supply-Common portal vein
precludes separation & also to evaluate
number and orientation of hepatic veins.Also
very useful in craniopagus.
• 4D-Easier for parents to understand & helps
in counselling.Better surface views
• But 2D and Doppler better to determine
degree of organ sharing
17. ROLE OF MRI
• Pre-surgical planning
- Fetuses stable on placental support
- No sedation required
- Defines degree of organ sharing
- T2WI excellent for brain/renal/chest detail
- Tl WI for additional bowel and liver information
• Clarify anomalies
- Either fetus may have lethal anomaly in addition
to being conjoined.
- Information may influence management
Termination of pregnancy.
Requirement for emergent separation.
Mode of delivery
18. PROGNOSIS
• The prognosis for conjoined twins is generally
unfavorable, with approximately 40% of cases
stillborn. The worst prognoses concern
craniopagus twins and those with a sole cardiac
mass. Structural anomalies are frequently
found such as polyhydramnios (50%), cardiac
malformations, common omphaloceles, and
neural tube defects. Upon discovery of nonviable
conjoined twins, interruption of pregnancy
should therefore be recommended
19. MANAGEMENT
• In the case of potentially viable conjoined twins, after
24 weeks GA the choice between vaginal delivery
or prophylactic caesarian section should be made
based on maternal safety and neonatal
criteria. Caesarian section avoids dystocia, uterine
rupture, and fetal death in utero.
• Approximately six to ten cases of conjoined twins per
annum worldwide are treated surgically. The surgery is
most successful when commonality of fetal organs is
limited; surgical intervention often takes place around
one year of age
20.
21. CONCLUSION
• Diagnosis of conjoined twins is possible as early
as 8 weeks GA, but accurate evaluation of
common structures is not possible. The 12-week
scan allows clinicians to assess viability, and, in
the case of nonviability, to propose early medical
interruption of pregnancy, preventing
hysterotomy in the case of a delayed
termination. Early discovery of viable conjoined
twins permits assessment of the best route of
delivery and a planning for serial sonography and
fast MRI to plan separation surgery
22. REFERENCES
•
•
•
•
•
•
•
•
•
1. Barth RA, Filly RA, Goldberg JD: Conjoined twins: Prenatal diagnosis and
assessment of associated malformations. Radiology 177:201-07, 1990.
2. Jirous J, Radocha K, Hanas S: Dicephalus, tribrachius: Prenatal diagnosis and
management. Acta Obstet Gynecol Scand 66:79-81, 1987.
3. Hammond DI, Okun NB, Carpenter BF: Prenatal ultrasonographic diagnosis of
dicephalus conjoined twins. Can Association Radiol J 42:357-9: 1991.
4. Apuzzio JJ, Ganesh VV, Chervenak J: Prenatal diagnosis of dicephalous conjoined
twins in a triplet pregnancy. Am J Obstet Gynecol 159:1214-5, 1988.
5. Fitzgerald EJ, Toi A, Cochlin DL: Conjoined twins: Antanatal ultrasound diagnosis
and a review of the literature. Br J Radiol 11:94-6, 1983.
6. Chatterjee MS, Weiss RR, Verma UL: Prenatal diagnosis of conjoined twins.
Prenat Diagn 3:357-61, 1983.
7. Guttmacher AF, Nichols BL: Teratology of conjoined twins. Birth Defects 3:3-9,
1967.
8. Chan DPC: Thoracompholapagus diagnosed before delivery. Med J Aust, I,
pp480-3, 1976.
9. Romero R, Pilu GL, Jeanty P: Prenatal diagnosis of congenital anomalies.
Appleton-Lange, Norwalk, 1988, p 405.