Seizure: Status Epilepticus
•Download as PPT, PDF•
70 likes•12,455 views

Seizure: Status Epilepticus: A comprehensive powerpoint Presentation by Dave Manriquez.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Seizure: Status Epilepticus
Similar to Seizure: Status Epilepticus (20)
More from Jack Frost
More from Jack Frost (20)
Recently uploaded
Recently uploaded (20)
Seizure: Status Epilepticus
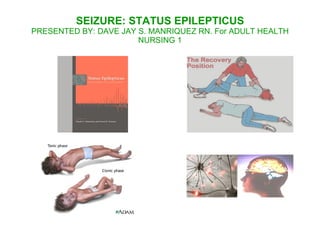
- 1. SEIZURE: STATUS EPILEPTICUS PRESENTED BY: DAVE JAY S. MANRIQUEZ RN. For ADULT HEALTH NURSING 1
- 2. SEIZURE sudden, excessive, disorderly electrical discharges of the neurons. EFFECTS OF SEIZURE: alteration in the following mental status LOC sensory and special senses motor funtion CLASSIFICATION OF SEIZURES A. Primary Generalized Seizure B. Partial Seizure GENERALIZED SEIZURES: GRAND MAL (Tonic-Clonic) most common type of seizure The phases are as follows: The phases are as follows:
- 4. PETIT MAL (Absence Seizure or Little Sickness) not preceeded by AURA little or no toni-clonic charac blank facial expression, automatism like lip-chewing, cheek smacking regain of consciousness as rapid as it was lot for 10-20secs usually occurs during childhood and adolescence JACKSONIAN / FOCAL SEIZURE common for patients with organic brain lesion like frontal lobe tumor aura is present(numbness, tingling, crawling feeling) charac by tonic-clonic movements of group muscle e.g. hands, foot, or face then it proceeds toi grand mal seizure FEBRILE SEIZURE this is common for children <5yo, when temp. is rising PSYCHOMOTOR SEIZURE aura is present (hallucinations or illusion) charac by mental clouding (being out of touch with the envt) appears intoxicated the client may commit violent or antisocial acts, e.g. Going naked public, running
- 5. PARTIAL SEIZURE 2 TYPES OF PARTIAL SEIZURES: A. Simple Partial Seizure B. Complex Partial Seizure Simple Partial Seizure Awareness Preserved Memory Preserved Consciousness Preserved
- 6. Complex Partial Seizure Awareness Preserved Memory Preserved Consciousness Preserved
- 7. CAUSES OF SEIZURES IN CHILDREN • Birth Traumas • Infections – Meningitis • Congenital Abnormalities • High Fever CAUSES OF SEIZURES IN MIDDLE YEARS • Head Injuries • Infections • Alcohol • Stimulant Drugs • Medications its Side Effects CAUSES OF SEIZURES IN THE ELDERLY • Brain Tumors • Strokes
- 8. CHEMICAL IMBALANCES CAUSE SEIZURE • Alcohol • Cocaine • Other Drugs • Low blood sugar, low oxygen, low blood sodium, low calcium, kidney and renal failure
- 9. Nursing Management During a Seizure - The nursing goal is to prevent injury to the patient. This includes not only physical support but psychological support as well. Provide privacy Ease the patient on the floor, if possible Protect the head with a pad to prevent injury Loosen constrictive clothing If aura precedes the seizure, place a padded tongue blade between the teeth Do not attempt to pry open jaws that are clenched in a spasm to insert anything No attempt should be made to restrain the patient during the seizure Place the patient on one side with head flexed forward The patent should be reoriented to the environments and happening upon awakening
- 10. Nursing Assessment during a Seizure - Observe and to record the sequence of symptoms. 3. Description of the circumstances before the attack. 4. The first thing a patient does in an attack. 5. The type of movements in the part of the body involved. 6. The size of both pupils. 7. Whether or not there is automatisms 8. Duration of each phase of the attack 9. Unconsciousness, ability to speak, consciousness
- 11. Epilepsy Disorders of brain function characterized by recurring seizures. Disturbance in consciousness, movement, behavior, mood, sensation, perception. It is not a disease but a symptom. Electrical disturbance in one section of nerve cells causing uncontrolled electrical discharges.
- 12. How is Epilepsy Diagnosed? History Physical Exam Electroencephalogram MRI (Neuro-imaging) CT Scan
- 13. 6 Truths about Epilepsy 1. Not to be called epileptic but a person with a seizure disorders 2. In epilepsy there might be seldom brain damage, brain function is disturb by seizure 3. Difference level of Intelligence 4. Violence does not follow epilepsy 5. Non usually inherited – cause is unknown and usually associated with environmental causes 6. Epilepsy is not a curse is a medical condition
- 14. Nursing Diagnoses • Fear related to the ever-present possibility of having seizures • Ineffective coping related to stresses imposed by epilepsy • Knowledge deficit about epilepsy and its control • High risk for injury during seizures
- 15. Goals: Short Term Goals: • Maintenance of control of seizures • Achievement of a satisfactory psychosocial adjustment • Acquisition of knowledge and understanding about the condition Long Term Goals: • To achieve a satisfactory life adjustment • To prevent or manage episodes of status epilepticus Nursing Interventions: • Seizure Control • Improved Coping Mechanisms • Patient Education
- 16. STATUS EPILEPTICUS (ACUTE PROLONGED SEIZURE ACTIVITY) IS A SERIES OF GENERALIZED SEIZURE THAT OCCUR WITHOUT FULL RECOVERY OF CONSCIOUSNESS BETWEEN ATTACKS THE TERM HAS BEEN BROADENED TO INCLUDE CONTINUOUS CLINICAL OR ELECTRICAL SEIZURES LASTING AT LEAST 30 MINUTES, EVEN WITHOUT IMPAIRMENT OF CONSCIOUSNESS. A seizure is a sudden disruption of the brain's normal electrical activity, which can cause a loss of consciousness and make the body twitch and jerk. This condition is a medical emergency.
- 17. CAUSES Not taking anticonvulsant medication Also caused by an underlying condition, such as meningitis, sepsis, encephalitis, brain tumor, head trauma, extremely high fever, low glucose levels, or exposure to toxins.
- 18. SymptomS The characteristic symptom of status epilepticus is seizures occurring so frequently that they appear to be one continuous seizure. These seizures include severe muscle contractions and difficulty breathing. Permanent damage can occur to the brain and heart if treatment is not immediate. A person's symptoms can range from simply appearing dazed to the more serious muscle contractions, spasms, and loss of consciousness. The specific symptoms depend on the underlying type of seizure.
- 19. TW C O ATEGORIES OF STATUS EPILEP US TIC CONVULSIVE Epilepsia partialis continua is a variant it involve an hour, day or even week-long jerking. It is a consequence of vascular disease, tumor or encepalitis and drug resistant. NONCONVULSIVE Complex Partial Status Epilepticus CPSE and absence status epilepticus are rare forms of the condition which are marked by nonconvulsive seizures. In the case of CPSE, the seizure is confined to a small area of the brain, normally the temporal lobe. But the latter, absence status epilepticus, is marked by a generalised seizure affecting the whole brain, and an EEG is needed to differentiate between the two conditions. This results in episodes characterized by a long-lasting stupor, staring and unresponsiveness.
- 20. NURSING DIAGNOSIS High Risk for Injury r/t Seizure Activity Individual Coping r/t perceive social stigma, potential changes in employment
- 21. HOW IT IS DIAGNOSED? Status epilepticus is diagnosed according to its characteristics symptoms. The doctor will order test to look for the cause of the seizures. This may include: Blood test ECG to check for an abnormal heart rhythm EEG to check electrical activity in the brain MRI or CT scan to check for braing tumord or signs of damage to the brain tissue.
- 22. MEDICATIONS Diazepam (Valium) this will stop motor movement Phenytoin (Dilatin) Phenobarbital (Barbita) Paraldehyde Thiopentahl sodium (Pentotal sodium) General anesthesia may also be used as a treatment of last resort to stop seizure activity
- 23. NURSING INTERVENTIONS PREVENTING INJURY REDUCING FEARS OF SEIZURE IMPROVING COPING MECHANISMS PROVIDING PATIENT AND FAMILY EDUCATION MONITORING AND MANAGING POTENTIAL COMPL TEACHING PATIENTS SELF-CARE
- 24. PREVENTING INJURY Injury prevention for the patient with seizure is a PRIORITY. patient should be placed on the floor and remove any obstructive items patient should never be forced into a position pad side rails do not attempt to pry open jaws that are clenched in a spasm to insert anything. if possible place the patient on one side with head flexed forward,
- 25. PATIENT EDUCATION TAKE MEDICATION AT REGULAR BASIS AVOID ALCOHOL. Lowers seizure threshold ADEQUATE REST WELL-BALANCED DIET AVOID DRIVING, OPERATING MACHINES, SWIMMING UNTIL SEIZURES ARE WELL CONTROLLED. LIVE AN ACTIVE LIFE
- 26. REDUCING FEARS OF SEIZURE Fear that a seizure may occur unexpectedly can be reduced by the patients adherence to the prescribed treatment regimen. Cooperation of the patient and family and their trust in the prescribed regimen are essential for control of seizures. Periodic monitoring is necessary to ensure the adequacy of the treatment regimen and to prevent the side effects..
- 27. IMPROVING COPING MECHANISMS It has been noted that the social, psychological, and behavioral problems frequently accompanying the attack can be more handicap than the actual seizure. Counselling assists the individual and family to understand the condition and the limitations imposed by it. Social and recreational opportunities are good for mental health . Nurses can improve the quality of life for patients with the disorder by educating them and their family about the symptom and also the management.
- 28. PROVIDING PATIENT AND FAMILY EDUCATION Ongoing education and encouragement should be given to patients to enable them to overcome these feelings. The patient and family should be educated about the medications as well as care during a seizure. Perhaps the most valuable facets are education and efforts to modify the attitudes of the patient and family toward the disorder.
- 29. MONITORING AND MANAGING POTENTIAL COMPLICATIONS Patients should have plan to have serum drug levels drawn at regular intervals. The patient and family are instructed about the side effects and are given specific guidelines to assess and report signs and symptoms indicating medication overdose.
- 30. TEACHING PATIENTS SELF CARE Like thorough oral hygiene after each meal, gum massage, daily flossing, and regular dental care. The patient is also instructed to inform all health care providers of the medication being taken because of the possibility of drug interactions. An individualized comprehensive teaching plan is needed to assist the patient and family to adjust to this chronic disorder.