Essentials of First Dialysis Session
•Download as PPTX, PDF•
35 likes•32,080 views

The document discusses factors to consider for a patient's first dialysis session for end-stage renal disease including using heparin-free anticoagulation, limiting fluid removal to 2 liters, using a bicarbonate dialysate, and having skilled medical staff present. It also provides guidelines for initial settings for a first session such as a blood flow rate of 150-200 ml/min, a dialysis time of 60-90 minutes, and a dialysate potassium level of 4-4.5 mmol/L. Precautions are recommended when initiating and terminating dialysis to ensure patient safety.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to Essentials of First Dialysis Session
Similar to Essentials of First Dialysis Session (20)
More from IPMS- KMU KPK PAKISTAN
More from IPMS- KMU KPK PAKISTAN (20)
Recently uploaded
Recently uploaded (20)
Essentials of First Dialysis Session
- 1. Yousaf khan Renal Dialysis lecturer IPMS-KMU
- 2. Planned dialysis for ESRD is very different to dialysis for an acute uremic emergency. In ESRD access may have been planned and formed several months previously, the patient is aware of the procedure and in general the metabolic derangement of CRF will have been progressing slowly. A first chronic dialysis session may be performed as a outpatient. However correction of metabolic abnormalities in ESRD can still have similar effect to that seen in HD for acute uremia. In ARF access will usually be temporary catheter, the patient may be confused, catabolic, sick or just frightened.
- 3. Factors to be considered include: Length of session, Blood flow rate Choice of dialyzer, Anticoagulation Dialysate composition, Fluid removal Skill of Technologist and presence of medical staff. Anticoagualtion: Heparin free dialysis is preferred for a first dialysis session, to minimize the risk of pericardial bleeding, bleeding from access sites, or intracerebral bleeding in the setting of hypertension. Anticaogulation can be introduce subsequently. Dialysis technologist and medical staff: A first dialysis session required skilled staffing for monitoring both the patient and equipment and for patient reassurance. Complication may be severe or unexpected.
- 4. Length of dialysis: A first dialysis should only reduce blood urea by 30 % For most patient an optimum first session is about 60 -90 minutes. Blood flow: Usually about 150 – 200ml/mint for the first dialysis session. Dialyzer: High efficiency dialyzer ( koA >400) are not needed for the first few dialysis session. If they are used, the length of session or blood flow should be reduced. Ultrafiltration: No more than 2 liter should be removed during a first dialysis session. For patient with severe fluid overload – isolated uf
- 5. Bicarbonate Preferred to acetate to minimize risk of hypotension. Patients at severe risk of alkalemia may need reduced bicarbonate concentration (<35mmol/l). Sodium: Avoid correction of hyponatremia too rapidly by altering the dialysate sodium. In general 140-145 mmol/l is satisfactory. Potassium: Serum potassium will be reduce with correction of acidosis. Use 4-4.5 mmol/l dialysate potassium. Calcium: Avoid low calcium dialysate as it may contribute to hypotension. Dialysate flow: Rate does not need altering (500 ml/mint)
- 7. General Reassessment: Acute and chronic dialysis prescription should be reviewed, evaluated and carried out accurately to obtain the maximal efficiency for dialysis. The patients physiologic status is assessed to ascertain the necessity of adjusting any dialysis orders. All machine parameters are assessed to ensure that the prescribed procedure is correctly implemented. The goal is to initiate and terminate the dialysis procedure safely and comfortably with no or minimal complication.
- 8. Through rinsing of the dialyzer is important because it may reduce the incidence or severity of anaphylactic dialyzer reaction by virtue of removal of leachable allergens. Micro bubbles are removed when the venous end of the dialyzer pointed upward. The dialyzer should be used within 5-10 minutes to avoid leaching of residual ethylene oxide or other leachable allergens into the rinsing fluid. Dialyzer should be rerinsed briefly immediately prior to dialysis if more than 10 minutes ha elapsed.
- 10. Weight, pulse rate, B.P laying and standing temperature, fluid status, blood investigation and vascular access patency and freedom from infection. Obtaining Vascular access: Poor vascular access is a limiting factor to patient survival on hemodialysis. Therefore great care must be taken to maintian adequate vascular access. Percutaneous venous cannula ( femoral, subclavian and jugular) Residual heparin or clot is first aspirated from both catheter lumen. Check the patency of each lumen by irrigating with a saline filled syringe. Heparin loading dose is administered in the venous limb and flushed with saline Initiate dialysis after 3 minutes. AVF and graft using permanent vascular access
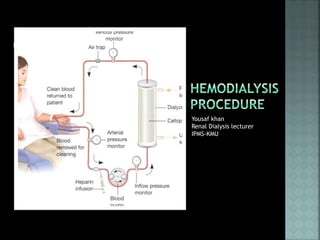
- 12. Set the blood flow rate at 50-100 ml/min, until the blood fills the blood circuit. The priming fluid in the lines and dialyzer is disposed of to drain until the blood reaches the venous air trap. in unstable patient the priming fluid is usually given to the patient maintain the blood volume. Increase the blood flow rate to the desired level after the circuit is filled with blood (150-250 in acute cases) Initiate the dialysis solution flow and adjust the TMP. Alarms: Blood circuit alarm and dialysis solution circuit alarms
- 13. Patient monitoring during dialysis Pulse rate, BP every 30 to 60 minutes in chronic dialysis, but at least every 15 minute in acute dialysis Food and fluid intake, complication during dialysis and particular observation. Termination of dialysis Saline rinse: The blood is returned by pumping sterile normal saline into the arterial side until the blood is displaced. After the bubble trap the fluid should be very pale pink in color ( to assure that the patient has lost the least of red cell) Saline air rinse: The blood is forced by pumping a small amount of saline into the arterial line, then the line is opened to allow air into the circuit to push the saline and blood. Again the fluid entering the patient should be very pale pink in color.
- 14. Patient monitoring post dialysis: Weight, pulse rate, BP laying and standing, Temperature, blood investigation and vascular access patency. All patient parameters and any unusual occurrences should be documented on patient file. Equipment care: The of dialysis machine is the responsibility of the staff and of the biomedical technicians. Scheduled maintenance recommended by the manufacturer should followed meticulously for the safe and efficient function of the equipment.