PDL, Cementum & Alveolar Bone
•Download as PPTX, PDF•
164 likes•49,731 views

This content consists of the Periodontal Ligament, Cementum and the Alveolar Bone discriptions. You can also find many content related captions over here. Thanks

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (8)
Similar to PDL, Cementum & Alveolar Bone
Similar to PDL, Cementum & Alveolar Bone (20)
Recently uploaded
Recently uploaded (20)
PDL, Cementum & Alveolar Bone
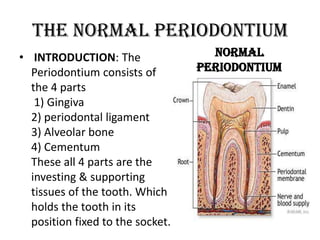
- 1. The Normal Periodontium • INTRODUCTION: The Normal Periodontium consists of Periodontium the 4 parts 1) Gingiva 2) periodontal ligament 3) Alveolar bone 4) Cementum These all 4 parts are the investing & supporting tissues of the tooth. Which holds the tooth in its position fixed to the socket.
- 2. PERIODONTAL LIGAMENT • The Periodontal Fiber or Periodontal Ligament, commonly abbreviated as the PDL ,is a group of the specialized connective tissue fibers that essentially attach a tooth to alveolar bone within which it sits. These fibers help the tooth withstand the naturally substantial compressive forces which occur during mastication(chewing) and remain embedded in the bone. It consists of bands of collagen fibers connecting the cement of the tooth to both gingival and alveolar bone and to the cement of adjacent teeth. Interspersed among the collagen fibers are loose connective tissue, blood vessels, lymphatic vessels, and nerves.
- 3. PERIODONAL FIBERS * The thickness of the periodontal ligament varies from tooth to tooth. * The thinnest portion of the PDL is near the middle of the root. * The width of the PDL shows a progressive decrease with age. * The most important thing to consider about PDL that it is always in a state of remodeling.
- 4. STRUCTURE OF PDL • It consist of cells, and extracellular compartment of fibers. The cells are fibroblast, epithelial, undifferentiated mesenchymal cells, bone and cementum cells. The extracellular compartment consists of collagen fibers bundles embedded in ground substance. The PDL substance has been estimated to be 70% water and is thought to have a significant effect on the tooth's ability to withstand stress loads. The PDL is a part of the periodontium that provide for the attachment of the teeth to the surrounding alveolar bone by way of the cementum.
- 5. PERIODONTAL FIBERS • The PDL collagen fibers are categorized according to their orientation and location along the tooth. 1. Transseptal fibers: extend interproximally over the alveolar bone crest and are embedded in the cementum of adjacent teeth; they form an interdental ligament. These fibers keep all the teeth aligned. These fibers may be considered as belonging to the gingiva because they don't have osseous attachment. 2. Alveolar crest fibers: extend obliquely from the cementum just beneath the junctional epithelium to the alveolar crest. These fibers prevent the extrusion of the tooth and resist lateral tooth movements. 3. Horizontal fibers: attach to the cementum apical to the alveolar crest fibers and run perpendicularly from the root of the tooth to the alveolar bone.
- 6. PERIODONTAL FIBERS 4. Oblique Fibers: are the most numerous fibers in the periodontal ligament, running from cementum in an oblique direction to insert into bone coronally. 5. Apical Fibers: radiating from cementum around the apex of the root to the bone, forming base of the socket. 6. Interradicular Fibers: Interradicular fibers are only found between the roots of multi-rooted teeth, such as molars. They also attach from the cementum and insert to the nearby alveolar bone.
- 7. FUNCTIONS OF PDL 1. It provides a support mechanism for the tooth; it cushions teeth against excessive occlusal forces, preventing damage to the blood vessels and nerves at the root apex. 2. It maintains the functional position of a tooth by keeping the teeth in contact and prevents the tooth from drifting or tilting. 3. The periodontal fibers undergo continuous change. Its cells form, maintain and repair the alveolar bone and cementum. 4. Sensors in the periodontal ligament provide proprioceptive input, detecting pressures on the tooth. 5. The periodontal ligament has a rich supply of blood, which provides nutrients to the cementoblasts.
- 8. • The width of the periodontal ligament ranges from 0.15 to 0.21 mm. • The part of the PDL fibers present in the cementum & alveolar bone are called Sharpey’s Fibers. • The fibroblasts, cementoblasts , osteoclast , undifferentiated mesenchymal cells, epithelial cells rest of malassez and osteoblasts are the synthetic cells of the PDL. • The macrophages, mast cells and lymphocytes are the defensive cells of the PDL. • The blood supply is through the branches from gingival vessels, intra-alveolar vessels & the apical vessels. • The Age Changes include the decrease in vascularity, cellularity and thickness. It may contain cementicles.
- 9. ALVEOLAR BONE An alveolar bone is a specialized type of bone which is designed to accommodate teeth. In humans, alveolar bone is found in the mandible, or lower part of the jaw, along with the maxilla, the upper part of the jaw. Alveolar bone is especially thick and dense when compared to other types of bone so that it can provide adequate support for the teeth, along with attachment points for muscles involved in the jaw and for the gums which provide protection for teeth and bone. This bone is also known as the “Alveolar Process”. It includes sockets which are designed to accommodate the roots and lower part of the teeth, with each socket separated from the next by an interdental septum.
- 10. ALVEOLAR BONE The gums attach to the alveolar process, and the bone has accommodations to allow blood vessels to enter for the purpose of supplying blood to the teeth. Damage to the alveolar bone can have serious consequences, including the risk of loss of teeth and septicemia if the damage is caused by an infection.
- 11. • ALVEOLAR SOCKET: It is also called dental alveolus. These are the sockets in the jaws in which the roots of teeth are held in the alveolar process with the periodontal ligament. • INTERDENTAL SEPTA: These are the plates of bone that separate each individual sockets from one another. • INTERTADICULAR SEPTA: These are the thin plates of bone that separate the roots of multi-rooted teeth. • CRIBRIFORM PLATE: Also called as bundle bone, is the compact layer of bone lining the tooth socket. • ALVEOLAR PROCESS: It is the thickened ridge of bone that contains the tooth sockets on bones that bear teeth.
- 12. cont’d alveolar bone . If the teeth are lost, the alveolar process disappears. . It is composed of two parts: 1) Alveolar bone proper & 2) Supporting bone. * Alveolar bone proper is that part of the alveolar bone that lines the socket. Radio graphically alveolar bone proper is referred to as LAMINA DURA. * The remainder of alveolar process below the alveolar bone proper is called Supporting bone. It is attached to the alveolar bone proper. It includes cortical plates and spongy bone.
- 13. CORTICLE PLATES: This is also called Compact Supporting Bone. The compact supporting bone of the alveolar process extends from the alveolar crest to the lower border of the socket on the outside surface of the maxilla & mandible. SPONGY BONE: This is also called Cancellous Bone. It is located apically between the alveolar bone proper and the cortical bone. Two types of bone are seen: 1) INTERDENTAL BONE: The bone between the roots of adjacent single-rooted or multi-rooted teeth is called Interdental Bone 2) INTERRADICULAR BONE: The bone between the roots of multi-rooted teeth is known as Interradicular Bone
- 14. AGE CHANGES IN ALVEOLAR BONE As people age, they often experience alveolar bone loss, which can be seen on dental x-rays. Sometimes the bone becomes thinner, and sometimes alveolar bone resorption occurs. In this case, part of the bone is reduced in volume. Resorption is often linked with damage to the jaw or the loss of teeth, which is one reason why extractions are avoided, if possible. Patients with severe damage may require alveolar bone grafting to replace missing bone or to promote bone growth to repair areas of damage. The alveolar bone forms a ridge around the neck of the tooth & holds properly in its socket.
- 15. FUNCTIONS OF ALVEOLAR BONE 1) PROTECTION: Alveolar bone forms and protects the sockets for the teeth. 2) ATTACHMENT: It gives the attachment to the PDL fibers, which are the principle fibers. These fibers which enter the bone are regarded as Sharpey’s Fibers. 3) SUPPORT: It supports the tooth roots on the facial & on the palatal/lingual sides. 4) SHOCK-ABSORBER: It helps absorb the forces placed upon the tooth by disseminating the force to underlying tissues.
- 16. VASCULAR SUPPLY OF ALVEOLAR BONE 1. ALVEOLAR PROCESS OF THE MAXILLA: Anterior & posterior alveolar arteries (branch from the maxilla & infra orbital arteries) 2. ALVEOLAR PROCESS OF THE MANDIBLE: a)Inferior alveolar arteries (internal) b) Periosteal branches of submental & buccal arteries (external).
- 17. CEMENTUM Cementum is the calcified, avascular mesenchymal tissue that forms the outer layer covering the anatomic root. 2 Types of the cementum are there: 1) Acellular cementum 2) Cellular cementum Composition of the cementum is: Organic portion is 50%, composed of collageneous & non- collageneous proteins while inorganic portion is 45-50% composed of hydroxyapatite crystals. The collageneous composition of the organic portion is type I (90%) & type III (5%). At cervical margin the thickness of cementum is 50um & at apical margin the thickness progresses to 200um.
- 18. CEMENTUM ACELLULAR CEMENTUM: It is the first cementum forms, covers approximately cervical third or half of the root & does not contain cells. CELLULAR CEMENTUM: It forms after the tooth reaches the occlusal plain. It is more irregular and contain cells (cementocytes) and in individual spaces (lacunae)
- 19. Cementum deposition is a continuous process that proceeds at varying rates. Cementum formation is most rapid in the apical regions where it compensates for the tooth eruption. The term hypercementosis refers to a prominent thickening of the cementum. The terminal apical area of cementum where it joins the internal root canal dentine is known as cemento-dentinal junction. The point or area where cementum joins the enamel is called cemento-enamel junction.
- 20. AGE CHANGES IN CEMENTUM Hypercementosis. Decrease permeability. Cementicles formation (which are round or ovoid calcified structures). Surface become rough. Cemental resorbtion More cemental deposition may leads to the closure of the apical foramen.
- 21. DIFFERENT B/W ACELLULAR & CELLULAR CEMENTUM ACELLULAR CEMENTUM CELLULAR CEMENTUM First formed Secondary formed Present on cervical 3rd or half Mainly on apical 3rd of root of the root It contains cells called It doesn’t contain cells cementocytes in lacunae It is formed before the tooth Formed after the tooth reaches reaches the occlusal plane the occlusal plane More calcified Less calcified Sharpey’s fibers are the main Sharpey’s fibers occupy smaller component and inserted at portion & are not the main right angles onto the root component. surface.