Cva
•
334 likes•190,567 views

This document discusses cerebrovascular disorders such as stroke. It begins by defining cerebrovascular disorders as any functional abnormality of the central nervous system caused by disrupted blood supply to the brain. Stroke is the primary cerebrovascular disorder. The document then covers the anatomy of the nervous system, definitions of stroke, risk factors, types of stroke (ischemic and hemorrhagic), clinical manifestations, diagnostic findings, and management approaches including medical, surgical, and nursing considerations.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (10)
Similar to Cva
Similar to Cva (20)
More from Nursing Path
More from Nursing Path (20)
Recently uploaded
Recently uploaded (20)
Cva
- 1. CEREBRO VASCULAR DISORDER (CEREBRO VASCULAR ACCIDENT) Dr. Jayesh Patidar www.drjayeshpatidar.blospot.com
- 2. INTRODUCTION • Cerebrovascular disorders” is any functional abnormality of the central nervous system (CNS) that occurs when the normal blood supply to the brain is disrupted. Stroke is the primary Cerebrovascular disorder in the United States and in the world. stroke is still the third leading cause of death. 30/04/2015 www.drjayeshpatidar.blogspot.com 2
- 3. ANATOMY & PHYSIOLOGY OF NERVOUS SYSTEM The nervous system is divided into two parts: • Central nervous system • Peripheral nervous system • ARTERIES: Two internal carotid arteries, Two vertebral arteries 30/04/2015 www.drjayeshpatidar.blogspot.com 3
- 4. DEFINITION • A stroke, or Cerebrovascular accident (CVA), occurs when blood supply to part of the brain is disrupted, causing brain cells to die. 30/04/2015 www.drjayeshpatidar.blogspot.com 4
- 5. INCIDENCE • AGE : The percentage is higher for people age 65 and older. Of those who survive, 50% to 70% will be functioning independent and 15% to 30% will live with permanent disability. • SEX : Stroke is more common in men than in women. 30/04/2015 www.drjayeshpatidar.blogspot.com 5
- 6. RACE • African american have a higher incidence of strokes than whites. • This high incidence may be related to increase rate of hypertension, diabetes mellitus and sickle cell anemia in african americans. • African americans also have a higher incidence of smoking and obesity than white, which are two other risk factors for stroke. • African american are twice as likely to die from a strokes as white. COUNTRY : • An estimated 700,000 person in the united states and 50,000 in canada suffer a stroke annually. • Stroke is the third most commen cause of the death in the united states and canada, behind cancer and heart disease. • In canada about 16,000 die from stroke each year, while in united states there are over 160,000 deaths from strokes. 30/04/2015 www.drjayeshpatidar.blogspot.com 6
- 7. ETIOLOGY Nonmodifiable risk factors : • Age : more than 65 yr • Gender : More in men than women • Race : African American • Family history : Heredity Modifiable risk factors : • Hypertension • Heart disease • Smoking 30/04/2015 www.drjayeshpatidar.blogspot.com 7
- 8. • Excessive alcohol consumption • Obesity • Sleep apnea • Metabolic syndrome • Poor diet • Drug abuse • Oral contraceptive 30/04/2015 www.drjayeshpatidar.blogspot.com 8
- 9. Causes • Vessel wall embolus • Carotid artery most often the source • Related to thrombus formation distal to stenosis • Cardiac source • Mitral valve stenosis • Mitral valve prolapsed • Calcified mitral annulus • Ventricular aneurysm • Atrial or ventricular clot • Valvular vegetation • Atrial septal defect 30/04/2015 www.drjayeshpatidar.blogspot.com 9
- 10. vascular sources • Intracranial artery thrombus (esp. African- Americans) • Aortic arch atherosclerotic Plaque • Transient hypotension with Carotid Stenosis 30/04/2015 www.drjayeshpatidar.blogspot.com 10
- 11. TYPES OF STROKE Strokes are classified as ischemic or hemorrhagic based on the underlying pathophysiologic findings. 30/04/2015 www.drjayeshpatidar.blogspot.com 11
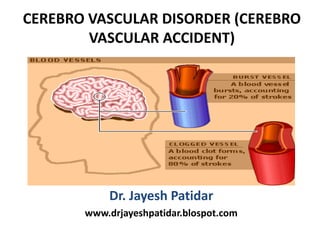
- 12. Ischemic stroke • An ischemic stroke result from inadequate blood flow to the brain from partial or complete occlusion of an artery. These account for approximately 80% of all strokes. Ischemic stroke are further divided into thrombotic and embolic. 30/04/2015 www.drjayeshpatidar.blogspot.com 12
- 13. Thrombotic stroke • A thrombotic stroke occurs from injury to a blood vessels wall and formation of a blood clot. The lumen of the blood vessel becomes narrowed and if it becomes occluded, infarction occur. Thrombosis develops readily where atherosclerotic plaques have already narrowed blood vessels. Thrombotic stroke, which is the result of thrombosis or narrowed blood vessel, is the most common cause of stroke. Two third of thrombotic strokes are associated with hypertension or diabetes mellitus 30/04/2015 www.drjayeshpatidar.blogspot.com 13
- 14. Embolic stroke • Another type of stroke may occur when a blood clot or a piece of atherosclerotic plaque (cholesterol and calcium deposits on the wall of the inside of the heart or artery) breaks loose, travels through the bloodstream and lodges in an artery in the brain. When blood flow stops, brain cells do not receive the oxygen and glucose they require to function and a stroke occurs. This type of stroke is referred to as an embolic stroke. 30/04/2015 www.drjayeshpatidar.blogspot.com 14
- 15. CLINICAL MANIFESTATIONS • Visual Field Deficits : Homonymous hemianopsia (loss of half of the visual field) - Unaware of persons or objects on side of visual loss - Neglect of one side of the body - Difficulty judging distances Loss of peripheral vision -Difficulty seeing at night - Unaware of objects or the borders of objects Diplopia -Double vision 30/04/2015 www.drjayeshpatidar.blogspot.com 15
- 16. Motor Deficits Hemiparesis • Weakness of the face, arm, and leg non the same side (due to a lesion in the opposite hemisphere) Hemiplegia • Paralysis of the face, arm, and leg on the same side (due to a lesion in the opposite hemisphere) Ataxia • Defective muscular co-ordination, unsteady gait Unable to keep feet together; needs a broad base to stand Dysarthria • Difficulty in forming words Dysphagia • Difficulty in swallowing 30/04/2015 www.drjayeshpatidar.blogspot.com 16
- 17. Sensory Deficits Paresthesia (occurs on the side opposite the lesion) • Numbness and tingling of Extremity 30/04/2015 www.drjayeshpatidar.blogspot.com 17
- 18. Verbal Deficits Expressive aphasia • Unable to form words that are understandable; may be able to speak in single-word responses Receptive aphasia • Unable to comprehend the spoken word; can speak but may not make sense Global (mixed) aphasia • Combination of both receptive and expressive aphasia 30/04/2015 www.drjayeshpatidar.blogspot.com 18
- 19. Cognitive Deficits • Short- and long-term memory loss • Decreased attention span • Impaired ability to concentrate • Poor abstract reasoning • Altered judgment Emotional Deficits • Loss of self-control • Emotional lability • Decreased tolerance to stressful situations • Depression • Withdrawal • Fear, hostility, and anger • Feelings of isolation 30/04/2015 www.drjayeshpatidar.blogspot.com 19
- 20. ASSESSMENT AND DIAGNOSTIC FINDING HEALTH HISTORY : • Past health history : Hypertension, previous stroke, aneurysm, cardiac disease (including recent myocardial infraction), dysrhythmias, heart failure, valvular disease, infective endocarditis, hyperlipidemia, polycythemia, diabetes • Family history : Hypertension, diabetes, stroke, coronary artery disease. • Medications : Use of oral contraceptives, use of antihypertensive and anticoagulant therapy • Nutritional history : Anorexia, nausea, vomiting,dysphagia, altered sensation of taste and smell • Cognitive perceptual history : Numbness, tingling of one side of body, loss of memory, altered in speech, pain, headache, visual disturbance 30/04/2015 www.drjayeshpatidar.blogspot.com 20
- 21. PHYSICAL ASSESSMENT • Glasgow coma scale • NIH stroke scale • COGNITIVE FUNCTION :- • Orientation : Speech :-aphasia & other problems – Fluent aphasia (motor/Borka’s) – inability to express self – Non-fluent aphasia ( sensory / wernicke’s) – inability to understand the spoken language. – Global aphasia – inability to speak or understand spoken language. – Other aphasia syndromes – amnesia, conduction. 30/04/2015 www.drjayeshpatidar.blogspot.com 21
- 22. • Other alterations include : – Confabulation – fluent , nonsensical speech – Preservation – continuation of thought process with inability to change rain of though without direction or repetition. • MOTOR FUNCTION : -Voluntary movement -Reflexive movement : Biceps, Triceps, Patellar, Achilles, Planter: 30/04/2015 www.drjayeshpatidar.blogspot.com 22
- 23. DIAGNOSTIC EVALUATION Diagnosis of stroke, including extent of involvement • CT, CTA (computer tomographic angiography) • MRI, MRA (magnetic resonance angiography) • SPECT (single photon emission computed tomography) • PET ( Positron emission tomography ) • MRS (magnetic resonance spectroscopy) • Xenon CT • Electroencephalogram • Cerebral angiography • Cerebrospinal fluid analysis 30/04/2015 www.drjayeshpatidar.blogspot.com 23
- 25. Cerebral blood flow measures • Cerebral angiography • Digital subtraction angiography • Doppler ultrasonography • Transcranial Doppler • Carotid duplex • Carotid angiography 30/04/2015 www.drjayeshpatidar.blogspot.com 25
- 26. Cardiac assessment • Electrocardiography • Chest x-ray • Cardiac enzymes • Holter monitor Additional studies • Complete blood count • Prothrombin time, activated partial thromboplastin time • Electrolytes • Blood glucose level • Renal and hepatic studies • Lipid profile • Arterial blood gases analysis 30/04/2015 www.drjayeshpatidar.blogspot.com 26
- 27. MANAGEMENT : MEDICAL MANAGEMENT : • Platelet-inhibiting medications : Aspirin, dipyridamole [Persantine], clopidogrel [Plavix], and ticlopidine [Ticlid]). Currently the most cost-effective antiplatelet regimen is aspirin 50 mg/d and dipyridamole 400 mg/d. • Thrombolytic therapy : Recombinant t-PA is a genetically engineered form of t PA, a thrombolytic substance made naturally by the body. The minimum dose is 0.9 mg/kg; the maximum dose is 90 mg. 30/04/2015 www.drjayeshpatidar.blogspot.com 27
- 28. Eligibility Criteria for t-PA Administration • Age 18 years or older • Clinical diagnosis of stroke with NIH stroke scale score under 22 • Time of onset of stroke known and is 3 hours or less • BP systolic ≤ 185; diastolic ≤ 110 • Not a minor stroke or rapidly resolving stroke • No seizure at onset of stroke • Not taking warfarin (Coumadin) • Prothrombin time ≤ 15 seconds or INR ≤ 1.7 • Not receiving heparin during the past 48 hours with elevated partial thromboplastin time. 30/04/2015 www.drjayeshpatidar.blogspot.com 28
- 29. • Platelet count ≥ 100,000 • Blood glucose level between 50 and 400 mg/dL • No acute myocardial infarction • No prior intracranial hemorrhage, neoplasm, arteriovenous, malformation, or aneurysm • No major surgical procedures within 14 days • No stroke or serious head injury within 3 months • No gastrointestinal or urinary bleeding within last 21 days • Not lactating or postpartum within last 30 days 30/04/2015 www.drjayeshpatidar.blogspot.com 29
- 30. Surgical management • Carotid endarterectomy : Removal of an atherosclerotic plaque or thrombus from the carotid artery to prevent stroke in patients with occlusive disease of the extracranial cerebral arteries. This surgery is indicated for patients with symptoms of TIA or mild stroke found to be due to severe (70% to 99%) carotid artery stenosis or moderate (50% to 69%) stenosis with other significant risk factors. 30/04/2015 www.drjayeshpatidar.blogspot.com 30
- 31. NURSING MANAGEMENT ASSESSMENT • Assess the level of consciousness or responsiveness as evidenced by movement, resistance to changes of position, and response to stimulation; orientation to time, place, and person • Presence or absence of voluntary or involuntary movements of the extremities; muscle tone; body posture; and position of the head • Stiffness or flaccidity of the neck • Eye opening, comparative size of pupils and pupillary reactions to light, and ocular position 30/04/2015 www.drjayeshpatidar.blogspot.com 31
- 32. • Color of the face and extremities; temperature and moisture of the skin • Quality and rates of pulse and respiration; arterial blood gas values as indicated, body temperature, and arterial pressure • Ability to speak • Volume of fluids ingested or administered; volume of urine excreted each 24 hours • Presence of bleeding • Maintenance of blood pressure within the desired parameters 30/04/2015 www.drjayeshpatidar.blogspot.com 32
- 33. NURSING DIAGNOSES • Impaired physical mobility related to hemiparesis, loss of balance and coordination, spasticity, and brain injury • Acute pain related to hemiplegia and disuse of extrimity • Self-care deficits (hygiene, toileting, grooming, and feeding) related to stroke • Disturbed sensory perception related to altered sensory reception, transmission, and/or integration • Impaired swallowing • Incontinence related to flaccid bladder, detrusor instability, confusion, or difficulty in communicating 30/04/2015 www.drjayeshpatidar.blogspot.com 33
- 34. • Disturbed thought processes related to brain damage, confusion, or inability to follow instructions • Impaired verbal communication related to brain damage • Risk for impaired skin integrity related to hemiparesis/ hemiplegia, or decreased mobility • Interrupted family processes related to catastrophic illness and caregiving burdens • Sexual dysfunction related to neurologic deficits or fear of failure 30/04/2015 www.drjayeshpatidar.blogspot.com 34
- 35. Hemorrhagic strokes • Hemorrhagic strokes account for 15% of cerebrovascular disorders and are primarily caused by an intracranial or subarachnoid hemorrhage • Hemorrhagic strokes are caused by bleeding into the brain tissue, the ventricles, or the subarachnoid space. Primary intracerebral hemorrhage from a spontaneous rupture of small vessels accounts for approximately 80% of hemorrhagic strokes and is primarily caused by uncontrolled hypertension 30/04/2015 www.drjayeshpatidar.blogspot.com 35
- 36. Pathophysiology Etiological factors • • presses on nearby cranial nerves or brain tissue • • • causing subarachnoid hemorrhage • • increase in ICP resulting from the sudden entry of blood into the subarachnoid space, • • injures brain tissue; or by secondary ischemia of the brain resulting from the reduced perfusion pressure 30/04/2015 www.drjayeshpatidar.blogspot.com 36
- 37. TYPE OF HEMORRHAGE • INTRACEREBRAL HEMORRHAGE An intracerebral haemorrhage, or bleeding into the brain substance, is most common in patients with hypertension and cerebral atherosclerosis because degenerative changes from these diseases cause rupture of the vessel. 30/04/2015 www.drjayeshpatidar.blogspot.com 37
- 38. • INTRACRANIAL (CEREBRAL) ANEURYSM An intracranial (cerebral) aneurysm is a dilation of the walls of a cerebral artery that develops as a result of weakness in the arterial wall. 30/04/2015 www.drjayeshpatidar.blogspot.com 38
- 39. • SUBARACHNOID HEMORRHAGE : • A subarachnoid hemorrhage (hemorrhage into the subarachnoid space) may occur as a result trauma, or hypertension. 30/04/2015 www.drjayeshpatidar.blogspot.com 39
- 40. CLINICAL MANIFESTATIONS • Severe headache • Loss of consciousness • Rigidity of the back and neck (nuchal rigidity) • Pain in spine due to meningeal irritation • Visual disturbance (visual loss, diplopia, ptosis) • Dizziness • Hemiparesis 30/04/2015 www.drjayeshpatidar.blogspot.com 40
- 41. ASSESSMENT AND DIAGNOSTIC FINDING : DIAGNOSTIC EVALUATION : • CT Scan : To determine the size and location of the hematoma as well as presence or absence of ventricular blood. • Cerebral angiography : To confirm the diagnosis of an aneurysm or AVM. • Lumber puncture PREVENTION: • Control hypertension. • Stop smoking. • Stop to take alcohol. • Avoid to take high cholesterol diet 30/04/2015 www.drjayeshpatidar.blogspot.com 41
- 42. SURGICAL MANAGEMENT • Craniotomy : Many patients with a primary intracerebral hemorrhage are not treated surgically. However, surgical evacuation is strongly recommended for the patient with a cerebellar hemorrhage if the diameter exceeds 3 cm. Surgical evacuation is most frequently accomplished via a craniotomy. 30/04/2015 www.drjayeshpatidar.blogspot.com 42
- 43. Extracranial-intracranial arterial bypass : An extracranial-intracranial arterial bypass may be performed to establish collateral blood supply to allow surgery on the aneurysm. Alternatively, an extracranial method may be used, whereby the carotid artery is gradually occluded in the neck to reduce pressure within the blood vessel. 30/04/2015 www.drjayeshpatidar.blogspot.com 43
- 44. POST OPERATIVE COMPLICATIONS : • Intraoperative embolization • Postoperative internal artery occlusion • Fluid and electrolyte disturbances 30/04/2015 www.drjayeshpatidar.blogspot.com 44
- 45. NURSING DIAGNOSIS : • Ineffective cerebral tissue perfusion related to bleeding • Disturbed sensory perception related to medically imposed restrictions (aneurysm precautions) • Anxiety related to illness and/or medically imposed restrictions (aneurysm precaution) 30/04/2015 www.drjayeshpatidar.blogspot.com 45
- 46. HOME CARE • Discuss measures to prevent subsequent strokes. • Identify signs and symptoms of specific complications. • Identify potential complications and discuss measures to prevent them (blood clots, aspiration, pneumonia, urinary tract infection, fecal impaction, skin breakdown, contracture). • Identify psychosocial consequences of stroke and appropriate interventions. • Identify safety measures to prevent falls. • State names, doses, indications, and side effects of medications. • 30/04/2015 www.drjayeshpatidar.blogspot.com 46
- 47. • Demonstrate adaptive techniques for accomplishing ADLs. • Demonstrate swallowing techniques (for patients with dysphagia). • Demonstrate care of enteric feeding tube, if applicable. • Demonstrate home exercises, use of splints or orthotics, proper positioning, and need for frequent repositioning. • Describe procedures for maintaining skin integrity. • Demonstrate indwelling catheter care, if applicable. Describe a bowel and bladder elimination program as appropriate. • Identify appropriate recreational or diversional activities, support groups, and community resources. 30/04/2015 www.drjayeshpatidar.blogspot.com 47