Tetrology of Fallot (TOF) - A Review
•Download as PPTX, PDF•
66 likes•6,950 views

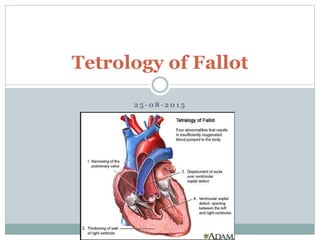
Tetralogy of Fallot (TOF) is a congenital heart defect characterized by four abnormalities: ventricular septal defect, pulmonary stenosis, overriding aorta, and right ventricular hypertrophy. It has been successfully repaired surgically since the 1950s. Current surgical repair in infancy has excellent outcomes, aiming to relieve right ventricular outflow tract obstruction. Long term complications can include pulmonary regurgitation and right heart dysfunction, but most TOF patients now survive well into adulthood thanks to advances in diagnosis and treatment.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to Tetrology of Fallot (TOF) - A Review
Similar to Tetrology of Fallot (TOF) - A Review (20)
Recently uploaded
Recently uploaded (20)
Tetrology of Fallot (TOF) - A Review
- 1. 2 5 - 0 8 - 2 0 1 5 Tetrology of Fallot
- 2. History Tetralogy of Fallot was first described by Niels Stenson in 1671, although its precise anatomical description was elegantly illustrated by William Hunter at St Georges Hospital Medical School in London in 1784. His description of a large outlet ventricular septal defect together with subpulmonary and pulmonary valve stenosis, and its resulting physiology, was refined by Etienne- Louis Fallot in 1888 in his description of L’anatomie pathologique de la maladie bleu, but the term tetralogy of Fallot is attributed to Canadian Maude Abbott in 1924.
- 4. Epidemiology About 3·5% of all infants born with a congenital heart disease have tetralogy of Fallot, corresponding to one in 3600 or 0·28 every 1000 livebirths, with males and females being affected equally. Its precise cause is unknown, as for most congenital heart diseases. Most cases seem sporadic, although the risk of recurrence in siblings is about 3% if there are no other affected first- degree relatives.
- 6. Genetic factors Monogenic or polygenic mode of inheritance. Autosomal dominant mode of inheritance with reduced penetrance, An autosomal recessive mode of inheritance, Multifactorial cause supporting the hypothesis that the genetic cause of TOF is heterogeneous. Environmental factors Maternal diabetes [threefold increased risk], Retinoic acids, Maternal phenylketonuria (PKU), and Trimethadione
- 7. Syndromes and associations DiGeorge/Velocardiofacial syndrome, Down syndrome, Alagille syndrome, Cat's-eye syndrome, recombinant chromosome (or San Luis Valley) and Kabuki syndromes, CHARGE and VATER/VACTERL associations, Poland syndrome and Goldenhar’s syndrome(oculo-auriculo- vertebral dysplasia). Microdeletion on 22q11….seen in 15–35% of TOF patients; 45% of TOF + PA; 65% of those with TOF + APV.
- 8. Embryology The aorta and pulmonary artery start as a single tube the truncus arteriosus which is then divided by the spiral septum. The spiral septum grows down to and attaches to the ventricular septum which isolates the left and right ventricles as well as isolating the aorta and pulmonary artery. However, if the spiral septum is not in the midline, but rather shifted over towards the right side of the heart, then what would happen? The opening to the aorta would be large The opening to the pulmonary would be small The spiral septum would “miss” the ventricular septum.
- 10. One abnormality results in 3 of the “defects” in TOF: "overriding” aorta (it opens up to both the right and left ventricles) pulmonary stenosis (the pulmonary artery is small and narrowed) VSD (because the spiral and ventricular septa do not line up and connect). The RV has to work extra hard to pump blood into the pulmonary artery and therefore hypertrophies to accommodate the extra work resulting in RVH. The pulmonary stenosis (PS) determines the degree of severity of this defect. Pulmonary perfusion depends on the size of the PS.
- 11. Anatomy Anterior and cephalad deviation of the infundibular septum. This results in a malaligned ventricular septal defect (VSD), with the aortic root overriding the defect and leading to subsequent right ventricular outflow obstruction. VSD is most commonly a single large malaligned subaortic defect located in the perimembranous region of the septum. The VSD can extend into the muscular septum. There are rarely other muscular ventricular septal defects.
- 12. RVOT Obstruction The right ventricular outflow obstruction is often at multiple levels. The anterior and cephalad deviation of the infundibular septum results in subvalvar obstruction Hypertrophy of muscular bands in this region can further accentuate subvalvar obstruction The pulmonary valve annulus is usually hypoplastic, although in some instances it is of normal size The pulmonary valve itself is frequently bicuspid and stenotic It is not uncommon to identify an area of supravalvar narrowing in the main pulmonary artery at the sinotubular ridge. There may also be further obstruction at the branch pulmonary arteries. These may be diffusely hypoplastic or have focal areas of stenosis, most commonly at the proximal branch pulmonary arteries.
- 16. Overriding aorta Aorta is displaced to the right over the VSD rather than the left ventricle. This results in blood flow from both ventricles into the aorta. The degree of aortic override of the VSD can vary widely and is one of the major factors used by some groups to differentiate between TOF and DORV. If one defines double outlet right ventricle as the presence of aortic/mitral valve fibrous continuity, then the degree of override is not relevant to diagnosis. If, however, one defines double outlet right ventricle as a condition with greater than 50 percent aortic override, then, by definition, the degree of aortic override in TOF is limited.
- 21. Pathophysiology The VSD is almost always large and non-restrictive in TOF, ensuring that the pressure is equal in the two ventricles. Consequently, the loud systolic murmur typical in affected infants originates from the dynamic narrowing of RVOT. The direction and magnitude of flow through the defect depends on the severity of the obstruction of RVOT. Most patients have adequate pulmonary blood flow at birth but develop increasing cyanosis during the first few weeks and months of life.
- 22. One of the physiologic characteristics of TOF is that the RVOT obstruction can fluctuate. An individual with minimal cyanosis can develop a dynamic increase in right ventricular outflow tract obstruction with a subsequent increase in right-to-left shunt and the development of cyanosis. In the most dramatic situation, there can be near occlusion of the right ventricular outflow tract with profound cyanosis. These episodes are often referred to as "tet spells" or "hypercyanotic spells".
- 23. Typical spell begins with progressive increase in rate and depth of respiration and culminates in paroxysmal hyperapnea, deepening cyanosis, limpiness, syncope and occasionally in convulsions, CVA and death. Peak incidence in between second and sixth month of life. Spells typically initiated by stress of feeding, crying or a bowel movement, particularly after awakening from deep sleep. Mechanisms - Acceleration in heart rate Increase in C.O. and venous return Increase in R→L shunt Vulnerable respiratory centre Infundibular contraction
- 25. Squatting
- 26. Complications Growth retardation Mental retardation Cerebral venous sinus thrombosis Nasal speech Brain abscess Cereberal embolism Infective endocarditis Coagulopathy Huperuricemia and Gout
- 27. Clinical features Wide due to variable severity of RV outflow obstruction USGfetal diagnosis Newborn & infants…cyanosis and systolic murmur. Acyanotic TOFmild pulmonary overcirculation rarely CHF unless there is a large PDA or aortopulmonary collateral arteries Pregnancy…poorly tolerated … gestational decrease in SVR increases R-L shunt & the labile SVR during labor, delivery leads to abrupt hypoxemia…..high fetal wastage / dysmature offspring.
- 28. Examination Cyanosis, Clubbing JVP is normal Arterial pulses …normal in uncomplicated TOF Wide pulse pressure (arterial diastolic runoff)…. aortopulmonary collaterals, palliative surgical shunt or PDA Accentuated precordial RV impulse LV impulse will not be hyperactive (normal cardiac output) S2 single& loud (anterior, dextroposed aorta) S3/S4 are unusual Aortic ejection click
- 29. Systolic murmur…crescendo-decrescendo @ LUSB. The intensity of the murmur inversely parallels the degree of pulmonic obstruction. Diastolic murmurs are unusual..Rarely AR murmur TOF with PA…..no harsh, obstructive precordial murmurs A harsh diastolic murmur, with a harsh murmur of PS, [harsh sawing, to-and-fro murmur ] ……TOF and APV syndrome Continuous murmurs….PDA, aortopulmonary collaterals, may be best heard in the back.
- 30. ECG
- 31. CXR
- 33. Echocardiography 2-D echocardiography provides the cornerstone for noninvasive diagnosis of TOF. Doppler analysis provides further data regarding hemodynamic characteristics. Study should be completed in a segmental and consistent manner that allows complete definition of the desired information. The coronary arteries are also readily apparent in PSAX view slightly superiorly. The origin and course of the left and right coronary arteries should be determined, paying special attention to whether any vessels take an anterior course across the infundibulum. Correct definition of the coronary artery anatomy was possible in most patients with a sensitivity of 82%, specificity of 99%, and accuracy of 98.5% in a study by Need et al.
- 36. LAD RCC NCC RCA LCx Pulm. Valve MPA The anomalous LAD crossing the RVOT in TOF is identified when the transducer is swept superiorly in the parasternal short -axis view . This allows visualization of the anomalous LAD that is situated anterior to the RVOT
- 37. Cardiac Catheterization With the evolution of noninvasive technology, the indications for diagnostic cardiac catheterization have diminished substantially. Nonetheless, invasive study to obtain both hemodynamic and anatomic information is, on occasion, helpful prior to deciding on surgical strategy. Foremost goal …. clarification or better definition of anatomic characteristics, such as pulmonary arterial or coronary arterial anatomy. Coronary artery anatomy … either by aortic root angio, selective coronary artery injection, or a combination of both.
- 40. A: An ascending aortogram in the LAO projection demonstrates a right anterior descending coronary artery arising from the right coronary artery. B: A selective left coronary injection shows filling of only the circumflex coronary artery.
- 41. Natural History
- 45. TREATMENT
- 46. The goal of management of TOF patients is to allow total surgical correction with minimal mortality and morbidity and to prevent or treat complications. Most newborns with TOF do not have ductal-dependent pulmonary blood flow and may be followed without specific early intervention. Depending of the severity of obstruction within the RV outflow tract, an infusion of prostaglandin may be initiated to preserve ductal patency, and provide a stable source of flow of blood to the lungs. IE Prophylaxis as per recommendations.
- 47. Hypercyanotic spells Treatment aims @ lowering impedance to pulmonary flow and further increasing systemic vascular resistance. Rx…..Oxygen, Volume expansion, Sedation with morphine or ketamine, and, if needed, vasopressors[phenylephrine] Refractory to above ….. Transfusion of whole blood/red cells Balloon angioplasty of pulmonary annulus Emergent surgical palliation or repair Propranolol …having some efficacy in minimizing or extinguishing the occurrence of spells. It may be used for patients who are awaiting surgical intervention or who have a medical contraindication to either complete repair or aortopulmonary shunt.
- 48. Timing of Surgery Palliative shunts were initially reserved for infants, and intracardiac repair for children, but the excellent results of intracardiac repair for neonates and infants have made it the current treatment of choice for all patients with TOF in most centers. Surgery is usually performed electively in the first year of life and can be performed in the first three months, if necessary. Intracardiac repair is also performed in asymptomatic acyanotic infants (pink variant) with a low morbidity and mortality; this approach may allow normal growth of the RVOT and pulmonary annulus.
- 49. Contraindications for repair in early infancy Palliation initially LAD from RCA crossing infundibulum Severely hypoplastic PAs Pulmonary atresia
- 50. Aim of surgery Relieving all possible sources of RVOTO. If possible, pulmonary valve function is preserved by avoiding a transannular patch. Closure of VSD (dacron patch) To relieve RVOTOpulmonary valvotomy, the insertion of an outflow tract patch or a transannular patch are often required. Surgery during early infancy, when the pulmonary annulus is markedly stenotic, frequently requires the insertion of a long and wide transannular patch. Consequently, most patients acquire PR as a result of the repair. PR may be well tolerated by many in the early postoperative years, but in the long term chronic PR is associated with reduced exercise capacity, RV dilatation, ventricular arrhythmias, and sudden death.
- 51. PA anatomy assessment 1) McGoon ratio: (Diameter of RPA/DAo + Diameter of LPA/DAo) Normal 2.1 Adequate for VSD closure 1.2 Inadequate <0.8 for VSD closure 2) Nakata Index:(CSA of RPA + CSA of LPA)/BSA Normal value > 200 mm2/m2 > 150 mm2/m2 is adequate. (Not usable preoperatively when MAPCAs are the major source of PBF & one- stage unifocalization + full repair is planned). 3) Total Neo-Pulmonary Artery Index (TNPAI) = APC index + Nakata Index APC index is the sum of CSA of all usable APCs/BSA >250 - suitable for one-stage repair including VSD closure (These pts. have low RV/LV pressure ratio postoperatively). 4) Z- score – no’s of SD PA size is away from the mean for children of same age and sex. Neaton’s number, Natio index, Blackstone index and Kugelberg angiographic classification.
- 53. Post Repair for TOF Current surgical survival, even for symptomatic infants <3 months of age, is excellent. Hospital and 1-month survival rates of 100% have been reported. Earlier age at repair (<1 year of age) did not adversely affect the rate of reintervention; so primary repair should be regarded as the preferred management strategy. Twenty-year survival for hospital survivors, irrespective of management strategy, was 98% for patients who have TOF with PS and slightly lower for patients with PA, reflecting the overall excellent long-term survival of these patients.
- 54. Complications Residual VSD Pulmonary regurgitation Residual RVOT obstruction RV wall motion abnormalities RV dysfunction and RHF Atrial tachycardia Ventricular tachycardia (VT)
- 55. Conclusions Tetralogy of Fallot is the most common form of cyanotic congenital heart disease, and one of the first to be successfully repaired by congenital heart surgeons. Since the first procedures in the 1950s, advances in the diagnosis, perioperative and surgical treatment, and postoperative care have been such that almost all those born with tetralogy of Fallot can now expect to survive to adulthood. The care of children with tetralogy of Fallot and their transition to adult life has been a success of modern medicine. Most of them now survive early repair and have an essentially normal childhood.
Editor's Notes
- GLH – Green Lane hospital, Auckland (NZ); UAB- University hospital Alabama(US)