B cell and T cell Neoplasms MADE easy
•Download as DOCX, PDF•
6 likes•2,782 views

An easy to remember and brief comparision of different kind of blood cancers. Considering most important points.

Recommended
More Related Content
Viewers also liked
Viewers also liked (20)
More from LWCH, UAE
Recently uploaded
Recently uploaded (20)
B cell and T cell Neoplasms MADE easy
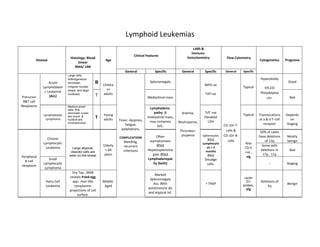
- 1. Lymphoid Leukemias LABS & Immuno- Clinical Features Histology: Blood histochemistry Flow Cytometry Disease Age Cytogenetics Prognosis Smear BMA/ LNB General Specific General Specific General Specific Large cells, heterogeneous Hyperploidy Acute chromatin, B Splenomegaly Good Childre MPO-ve Lymphoblasti irregular nuclear Typical t(9,22) shape, and large n> c Leukemia Philadelphia nucleolus. T adults TdT+ve Precursor (ALL) Mediastinal mass Bad chr. B&T cell Neoplasms Medium-sized cells ,fine Lymphadeno- chromatin nuclei pathy & Anemia, TdT +ve Lymphoblastic Young Typical Translocations Depends Lymphoma are round & T adults mediastinal mass, Elevated at a & d T-cell on nucleoli are Fever, dyspnea, may compress LDH inconspicuous. Neutropenia, receptor Staging fatigue, SVC. CD-10< T- palpitations, cells & Thromboc- 50% of cases Often ytopenia Spherocytes CD-10> B- have deletions Mostly Chronic COMPLICATIONS asymptomatic (CLL) cells of 13q benign Lymphocytic Bleeding, Lymphocyto Also Elderly recurrent (CLL) Some with Leukemia Large atypical, sis > 3 CD-5 > 60 infections Hepatosplenome months deletions in Bad cleaved cells are +ve , seen on the smear years galy. (CLL) (CLL) 17p , 11q Peripheral sIg Small Lymphadenopat Smudge B-cell Lymphocytic hy (both) cells. -- Staging neoplasm Lymphoma Dry Tap , BMB Marked reveals Fried-egg cyclin Splenomegaly Hairy Cell app. ,Hair-like Middle- D1 Deletions of Ass. With + TRAP protein, Benign Leukemia cytoplasmic Aged 5q autoimmune dis sIg projections of cell and atypical Inf. surface.
- 2. MYELOID Leukemias LABS & Disease Immuno- Histology: Risk Clinical Features Of Type Age histochemistry Flow cytometry Cytogenetics Prognosis BMA Factors BoneMarrow General Specific General Specific M3 or (Acute Alkylating Fever, dyspnea, MPO or Anemia, t(15;17) Good promyelocytic agents, fatigue, May develop DIC Sudan leukemia) is palpitations Acute MC type. and cells may Neutropenia, Black +ve MDS, Auer-rods Myelogenous Have numerous infiltrate tissues , intra-cytoplasmic COMPLICATIONS on CD-33 +ve Normal gene Bad Leukemia Any Age graulocytic Thromboc- granules , Poly.Vera, Bleeding, peripheral (AML) Group, sarcoma, ytopenia Called Auer-rods, Recurrent blood smear Myeloid MC gingivitis & >50% blasts on Aplastic infections Neoplasms BMA elderly Anemia Elevated PT -5, -7 worse Hypercellular bone Anemia Chronic with all cell lines fever, weight loss Depends increased in no. due t(9;22) Myelogenous ionizing Massive Variable Decreased on to clonal expansion ----- Philadelphia Leukemia of pluripotent stem radiation COMPLICATION splenomegaly platelets LAP Sokal chr. (CML) cells Bleeding, score Leukocytosis
- 3. Non Hodgkin Lymphoma (NHL): Lymphomas are tumors originating in the Lymph nodes Peripheral T-cell Peripheral B-cell neoplasm Neoplasm Diffuse Large Small non- B-cell Lymphoma Small cleaved cell Cut. T-cell cleaved Follicular Lymphoma Marginal Zone Lymphoplasmacytic Lymphoma Disease Lymphoma Lymphoma Immuno- (Mantle cell Lymphoma Lymphoma Mycosis Fungiodes Body- (Burkitt deficiency Lymphoma) (MC) cavity Lymphoma) associated Age Median Age 6th decade , Young adults ( Burkitt) High grade Malignant CD4 T- Histology: Well differentiated Malignant B-cells, B-cell neoplasm High-grade Large B-cell Intermediate B- cell with nuclei that Bone Marrow asp. B-cell neoplasm arising from the arise from Small B-lymphocytes showing neoplasm with diffuse cell Neoplasm are hyperchromatic /Lymph Node asp. or with follicular mantle zone of Lymphatic tissue plasmacytic differentiation growth pattern with starry sky and convoluted or involved site pattern of growth Lymph nodes of GIT app. cerebriform. Peripheral adenopathy (except MALT) , Fever, night sweats, weight loss and weakness , Extra-nodal involvement in High grade lymphomas Anorexia, Abdominal Constipation, Generalized pruritic Clinical Presentations tenderness and Generalized lymph- tarry stools, erythematous Rash Infiltration of LN spleen Disseminated LN abdominal mass adenopathy dyspnea (SS) , Pautrier EBV HHV-8 (hepatosplenomegaly) and spread (HIV) & Massive Ass. With as microabscess, May bonemarrow (HCV) Mandibular or Spleomegaly Sjogren dis. or H. be associated with maxillary mass pylori gastritis HTLV-1 (EBV) neutropenia, anemia, thrombocytopenia, Elevated LDH, Hyperuricemia Lymphocytosis (low-grade) LABS IgM spike , Elevated ESR, Peripheral CBC Typical Typical Typical + Lymphocytosis Typical Rouleaux formation , BJ reveal CD4 T-cells proteins in urine AKA Sezary Cells Cytogenetics t(14;18) Random t(8;14) t(11;14) t(11;18) Deletions of 6q ----- Typical : CD-10< T-cells, CD-10 > B-cells and sIg Flow cytometry Typical Typical Typical CD 5 also CD 20 mostly Typical Typical Complications Spinal cord compression , Superior vena cava (SVC) syndrome , Infection, Bleeding , GI obstruction, perforation (MALT) , visual problems (LL) Prognosis Depends on Staging