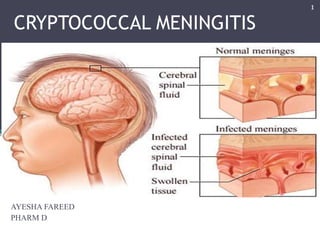
Cryptococcal meningitis is caused by the fungus Cryptococcus infecting the brain and spinal cord. It commonly affects people with weakened immune systems. Symptoms include headache, fever, neck stiffness, nausea and altered mental status. Diagnosis involves examining cerebrospinal fluid for cryptococcal antigen or viewing yeast cells with India ink stain. Treatment involves antifungal medications like amphotericin B and fluconazole given over several weeks to months depending on severity and patient's immune status.
2. The genus Cryptococcus contains at least 39 species of yeast, but few are able to cause
disease in humans.
Most human infections are due to C. neoformans.
Infection with the fungus Cryptococcus (either C. neoformans or C. gattii) is called
cryptococcosis.
Cryptococcosis is a global invasive mycosis associated with significant morbidity and
mortality.
Cryptococcosis usually affects the lungs or the central nervous system (the brain and
spinal cord), but it can also affect other parts of the body.
Brain infections due to the fungus Cryptococcus are called cryptococcal meningitis.
Cryptococcus neoformans is a fungus that lives in the environment throughout the
world.
2
3. 3
Cryptococcus neoformans is
dimorphic, existing in the asexual
yeast form characterized by oval to
spherical cells with a
polysaccharide capsule, and in the
sexual or perfect state characterized
by the presence of basidiospores.
C. neoformans is readily cultured in
the laboratory, producing mucoid
colonies within 36–72 h, although
growth is inhibited at 37 °C.
Colonies are white to cream in
colour, but characteristic dark
brown colonies are formed when
grown on birdseed agar.
5. 5
C. neoformans infections are not contagious. Humans and animals can get the
infection after inhaling the microscopic fungus from the environment.
Meningitis is the most common manifestation of cryptococcal infection.
The lung is the second most common organ to develop clinical disease, usually
pneumonia, which can occur in the immunocompetent
The skin is the third most common organ to be affected by cryptococcal infection
6. EPIDEMIOLOGY
Cryptococcosis is a rare infection in healthy human population
C. neoformans is a major cause of illness in people living with HIV/AIDS, with an
estimated 1 million cases of cryptococcal meningitis occurring worldwide each year.
Most cases occur in the 20–50 years old age group.
Global burden of HIV-related cryptococcal meningitis
6
7. Causes of death in sub-Saharan Africa, excluding HIV/AIDS
7
9. Most cases of C. neoformans infection occur in people who have weakened immune
systems, such as people who:
• Have advanced HIV/AIDS,
• Have had an organ transplant
• Sarcoidosis;
• Lymphoproliferative disorder;
• Hypogammaglobulinaemia;
• Systemic lupus erythematosus;
• Cirrhosis;
• Peritoneal dialysis
• Are taking corticosteroids, medications to treat rheumatoid arthritis, or other
medications that weaken the immune system.
WHO ARE AT RISK?
9
10. In the BRAIN (cryptococcal meningitis)
Cryptococcal meningitis is an infection caused by the fungus Cryptococcus after it
spreads from the lungs to the brain. The symptoms of cryptococcal meningitis
include:
• Headache
• Fever
• Neck pain; neck rigidity
• Nausea and vomiting, lethargy, personality change, memory loss
• Sensitivity to light
• Confusion or changes in behavior
• The duration of symptoms before presentation is likely to be longer in non-AIDS
patients, with a history of more than 2 weeks in only 25% of HIV positive
patients.
CLINICAL PRESENTATION:
10
11. DIAGNOSIS :
Definitive diagnosis of cryptococcal meningitis requires lumbar puncture with
demonstration of yeasts with India ink stain, positive cryptococcal antigen testing or
culture of the organism.
CSF EXAMINATION:
CSF examination generally reveals a mild mononuclear leucocytosis (50–500
cells/μL).
The CSF protein is rarely greater than 500–1000 mg/Dl and it may be normal,
especially in HIV patients.
In HIV patients, the cell count is usually much lower, and often in single figures.
11
12. 12
IMAGING:
CT brain scan is normal in 50% of patients with cryptococcal meningitis. The most
common abnormal finding is hydrocephalus
Magnetic resonance imaging is more likely to demonstrate abnormalities than CT
Scanning.
DIAGNOSTIC TECHNIQUES:
India ink test
The CSF India ink test is a simple and relatively sensitive test that enables the rapid
diagnosis of cryptococcal meningitis.
Yeast cells are easily identified through the halo effect that occurs around them
because of the glucuronoxylomannan capsule.
A concentration of yeasts less than 104 colony forming units (CFU) is unlikely to be
detected.
14. 14
CULTURE
C. neoformans from CSF or blood grows readily on blood or Sabouraud’s agar at 35
°C. Identification can be confirmed through the demonstration of capsule growth on
corn meal agar, development of characteristic brown mucoid colonies on birdseed
agar, and through commercially available sugar assimilation test kits.
C. neoformans grows easily in commercially available automated blood culture
systems. Culture of CSF is more sensitive in detecting cryptococcal infection than the
India ink test, with a sensitivity approaching 90%.
CRYPTOCOCCALANTIGEN
Cryptococcal antigen testing is both sensitive and specific in identifying patients with
cryptococcal disease.
The kits can be used on serum or CSF and the sensitivity in CSF is greater than 90%
in cryptococcal meningitis.
SEROTYPING
There are immunotyping kits to distinguish the various cryptococcal serotypes.
However, they are expensive.
16. 16
TREATMENT
Anti-fungal drug options for cryptococcal disease are limited.
There are three phases – induction, consolidation and maintenance (also known as
secondary prophylaxis).
17. 17
Continuation of combination induction therapy beyond 2 weeks may be considered if:
(1) A patient remains comatose;
(2) The patient is clinically deteriorating;
(3) The patient has not improved, with persisting elevated, symptomatic intracranial
pressure; and/or
(4) The results of CSF culture obtained after 2 weeks of induction therapy is
anticipated to remain positive.
These patients may require additional weeks (eg, 1–6 weeks) of the induction phase of
treatment.
Maintenance (suppressive) and prophylactic therapy:
Maintenance therapy should be initiated after completion of primary therapy with an
induction and consolidation regimen.
18. 18
ORGAN TRANSPLANT RECIPIENTS:
Regimen Duration Evidence
Induction therapy:(a)
liposomal AmB (3–4 mg/kg per day) or
ABLC (5 mg/kg per day) plus flucytosine (100 mg/kg per
day)
2 weeks B-III
Alternatives for induction therapy:
Liposomal AmB (6 mg/kg per day) or ABLC (5 mg/kg per
day)
4–6 weeks B-III
AmBd (0.7 mg/kg per day)b 4–6 weeks B-III
Consolidation therapy:
fluconazole (400–800 mg per day)f 8weeks B-III
Maintenance therapy:
fluconazole (200 mg per day)b 6 - 12weeks B-III
a Immunosuppressive management may require sequential or step-wise reductions.
b Many transplant recipients have been successfully treated with AmBd; however,
issues of renal dysfunction with calcineurin inhibitors are important and the effective
dose is imprecise.
19. 19
Regimen Duration Evidence
Induction therapy:
AmBd (0.7–1.0 mg/kg per day) plus flucytosine (100
mg/kg per day)
≥4 weeks a,b B-II
AmBd (0.7–1.0 mg/kg per day)c ≥6 weeks a,b B-II
Liposomal AmB (3–4 mg/kg per day) or ABLC (5 mg/kg
per day) combined with flucytosine, if possible d
≥4 weeks a,b B-III
AmBd (0.7 mg/kg per day) plus flucytosine (100 mg/kg
per day)e
2 weeks B-II
Consolidation therapy:
fluconazole (400–800 mg per day)f 8weeks B-III
Maintenance therapy:
fluconazole (200 mg per day)b 6 - 12weeks B-III
Non–HIV Infected and Nontransplant Patients:
20. 20
a Four weeks are reserved for patients with meningitis who have no neurological
complications, who have no significant underlying diseases or
immunosuppression, and for whom the cerebrospinal fluid culture performed at
the end of 2 weeks of treatment does not yield viable yeasts; during the second
2 weeks, lipid formulations of AmB may be substituted for AmBd.
b Fluconazole is given at 200 mg per day to prevent relapse after induction
therapy, and consolidation therapy is recommended.
c For flucytosine-intolerant patients.
d For AmBd-intolerant patients.
e For patients who have a low risk of therapeutic failure. Low risk is defined as
an early diagnosis by history, no uncontrolled underlying condition or
severe immunocompromised state, and an excellent clinical response to initial 2-
week antifungal combination course.
f A higher dosage of fluconazole (800 mg per day) is recommended if the 2-week
induction regimen was used and if there is normal renal function
21. 21
NONMENINGEAL CRYPTOCOCCOSIS
Patient group Initial antifungal
regimen
Duration Ev.
Immunosuppressed patients and
immunocompetent
patients with mild-to-moderate pulmonary
cryptococcosis
Fluconazole (400
mg per day)
6–12
months
B-III
Immunosuppressed patientsa and
immunocompetent patients
with severe pulmonary cryptococcosis
Same as CNS
disease
12 months B-III
Patients with nonmeningeal, nonpulmonary
cryptococcosis
Patients with cryptococcemia Same as CNS
disease
12 months B-III
Patients for whom CNS disease has been
ruled out with no fungemia, with a single
site of infection, and with no
immunosuppressive risk factors
Same as CNS
disease
6-12
months
B-III
A Should directly rule out CNS disease with lumbar puncture.
22. 22
REFERENCES:
1. John R. Perfect, et.al. Clinical Practice Guidelines for the Management of
Cryptococcal Disease: 2010 Update by the Infectious Diseases Society of
America.
2. Jeremy N Day Clinical Research Fellow, Oxford University Clinical Research
Unit, Hospital for Tropical Diseases, 190 Ben Ham Tu, Quan 5, Ho Chi Minh
City, Viet Nam; Practical Neurology, 2004, 4, 274–285.
3. Southern African HIV Clinicians Society, Guideline for the prevention,
diagnosis and management of cryptococcal meningitis among HIV-infected
persons: 2013 update , S Afr J HIV Med 2013;14(2):76-86.
DOI:10.7196/SAJHIVMED.930
4. http://www.cdc.gov/fungal/diseases/cryptococcosisneoformans/