
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Ocular Lymphoma Guide
Similar to Ocular Lymphoma Guide (20)
Recently uploaded
Recently uploaded (20)
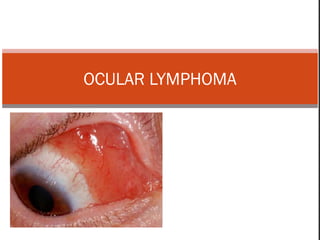
Ocular Lymphoma Guide
- 2. Lymphoid tumors represent ~10% of biopsy-proven orbital disorders Lymphatic tissues do not exist in orbit. Point of dispute Orbit contains scattered lymphocytes. 06/14/15
- 3. 06/14/15
- 4. 06/14/15 Ocular lymphoma Orbit is an extranodal site Depending on the site of involvement, Orbital Adnexal Intraocular
- 5. Distribution of common lymphoproliferative lesions of the orbit.
- 6. 06/14/15 Ocular manifestations Frequently masquerade as other more benign intraocular conditions Proptosis Visible conjunctival mass Allergic or infectious conjunctivitis Uveitis Multiple evanescent white dot syndrome Acute retinal necrosis Herpetic retinitis.
- 7. Orbital & Adnexal lymphoma 06/14/15
- 8. 06/14/15 Orbital and ocular adnexal lymphoma Insidious onset Progress over a year before producing symptoms. Symptoms :20 to pressure effects on surrounding structures. Clinical features Painless proptosis with or without motility disturbances Double vision Ptosis Decreased vision.
- 9. 06/14/15 Orbital and ocular adnexal lymphoma Unilateral or bilateral. More common in the anterior superior orbit. Preseptal portion of the eyelid can be involved. Usually rubbery to firm on palpation No palpable bony destruction. The lacrimal gland, lacrimal sac, EOM can be similarly involved.
- 10. 06/14/15 Systemic disease to be suspected Cervical lymphadenopathy, Preauricular lymphadenopathy Parotid gland swelling Abdominal mass Thorough physical evaluation
- 11. Of primary orbital lymphoid lesions, 50% reactive or atypical hyperplasia 50% malignant lymphoma. Recent evidence, show systemic disease occurring in 15% to 25% of reactive hyperplasias, 40% of atypical hyperplasias, 20% of well-differentiated lymphomas, and 60% of poorly differentiated lymphomas.
- 12. Reactive lymphoid hyperplasia of the bulbar conjunctiva and upper fornix. Appearance is similar to that of malignant lymphoma.
- 13. Lymphoid tumor (malignant lymphoma) of bulbar conjunctiva. Tumor involves inferior bulbar and forniceal conjunctiva
- 14. (a) Anterior epibulbar extension of a deeper orbital lymphoma. (b) The computed tomography (CT) scan reveals a large molding soft tissue mass tracking along the medial orbit and extending onto the epibulbar surface of the LE.
- 15. (a) Bilateral lymphoid lesions of the preseptal portion of the eyelid. On palpation, the lesions had a doughy consistency. (b) CT scan demonstrates masses involving the eyelids and anterior orbit. The clinical examination is therefore important in the correct interpretation of these findings.
- 16. 06/14/15 Differential diagnosis of orbital lymphoma Idiopathic inflammatory pseudotumor Orbital lymphoid hyperplasia Orbital sarcoidosis Wegener granulomatosis Chronic dacryoadenitis.
- 17. Lymphoma of the lacrimal gland Painless mass Characteristic salmon-colored mass seen in the superolateral cul- de-sac, Often fixed to the orbital rim and is rubbery Radiographic appearance of the bone is usually normal CT scan a homogeneous consistency with indistinct borders Tendency to mold into the contour of the lacrimal fossa and the surrounding bony contour.
- 18. Bilateral painless enlargement of the lacrimal glands leading to mechanical ptosis. Intraoperative photo shows the enlarged lacrimal gland. After chemotherapy for systemic lymphoma.` Fish flesh appearan
- 19. lymphoma Conjunctiva Lacrimal gland Tend to be more benign ,better long-term prognosis Those that extend into the orbit tend to be more malignant. Remain localized in 90% of cases Appear as a diffuse vertical expansion of the gland, Mold to both the globe and orbital bone No bony fossa erosion.
- 20. Conjunctival lymphoid ‘salmon-patch’ lesion. This lymphoid tissue is located within the substantia propria of the conjunctiva and is freely mobile over the underlying tunics.
- 21. NON HODGKINS B CELL LYMPHOMAS 06/14/15
- 22. Subtypes of B-cell nonHodgkin's malignant lymphoma— 1. Extranodal B-cell marginal zone lymphoma, 2. Follicle center cell lymphoma, 3. Small lymphocytic lymphoma, 4. Lymphoplasmacytoid lymphoma, 5. Large cell lymphoma, 6. Mantle cell lymphoma, 7. Burkitt's lymphoma
- 23. 1. EXTRANODAL B-CELL MARGINAL ZONE LYMPHOMA Most common type Both conjunctival and lacrimal gland MALT contribute lysozyme to the tear film. Chlamydia psittaci is associated with ocular adnexal mucosa-associated lymphoid tissue (MALT) lymphoma
- 24. FOLLICULAR LYMPHOMA 06/14/15 • Is relatively rare • Middle-aged to elderly • Females • Relapses are frequent • Long-term survival: favorable JAMA Ophthalmol. doi:10.1001/jamaophthalmol.2014.376 Published online April 24, 2014. , A uniform population of small cells (centrocytes) with irregular nuclei (arrows) consistent with a grade 1 follicular lymphoma follicles express CD10,
- 25. B CELL-CHRONIC LYMPHOCYTIC LEUKEMIA SMALL LYMPHOCYTIC LYMPHOMA Predominantly a disease of the elderly Present with leukemia involving the orbit Relatively indolent disease, but it is virtually incurable with current therapy May progress to a higher grade large cell lymphoma (richter transformation).
- 26. LYMPHOPLASMACYTOID LYMPHOMA Occurs in elderly Paraproteinemia is common Hyperviscosity state The optic nerve can be invaded Papilloedema from CNS invasion Resembles lymphoma in its diffuse infiltration into lymphoid tissues. Bone marrow Biopsy: characteristic mixture of small lymphoid cells with various degrees of plasma cell differentiation.
- 27. PLASMA CELL TUMORS Tumors of mature B cells Secrete monoclonal immunoglobulin detected as the M-spike on serum electrophoresis, associated with high urine and blood content of immunoglobulin. Light chain fragments excreted in the urine are known as Bence Jones protein.
- 28. Multiple myeloma Prototypic systemic plasma cell tumor Occurs in the elderly, more commonly men Multiple masses of plasma cells disseminated throughout the skeletal system and soft tissue. Extraskeletal metastases in 70% of cases, either by hematogenous spread or by direct extension. Metastasize to the kidney, adrenal gland, heart, and liver Punched-out lesions of the skull and vertebral fractures.
- 29. LARGE CELL LYMPHOMA 06/14/15 • Worst prognosis for survival. • Death occurs within 2 years of diagnosis JAMA Ophthalmol. doi:10.1001/jamaophthalmol.2014.4644 Published online November 13, 2014. High Ki-67 proliferative index exceeding 90% (yellow arrowhead) (original magnificatio n ×400).
- 30. Burkitt’s lymphoma A rare tumor Originally described in africa. Most common in children Comprising 90% of pediatric lymphomas in endemic regions and one third of nonendemic pediatric lymphomas.. •In the orbit, it typically originates from the maxillary marrow space. •Rapid tumor growth in the face, with a doubling time of 3 days •Tumor of monstrous proportion in 2 to 4 weeks "starry sky“ appearance. B, At high power, -monotonous appearance
- 31. Management of Burkitts lymphoma Chemotherapy regimens based on cyclophosphamide, doxorubicin, vincristine, and methotrexate. Prognosis depends on the volume of disease at presentation, If the disease is localized, it can be surgically debulked. Fifty percent of tumors recur, commonly in the meninges. Aggressive disease with meningeal invasion - chemotherapy with bone marrow transplant.
- 32. Mantle cell lymphoma 06/14/15 A, At low power, neoplastic lymphoid cells surround a small, atrophic germinal center, exhibiting mantle zone pattern of growth. B, High-power view shows a homogeneous population of small lymphoid cells with somewhat irregular nuclear outlines, condensed chromatin, and scant cytoplasm.
- 34. HODGKIN'S LYMPHOMA 30% of all systemic lymphomas, Is rare in the orbital soft tissues and lacrimal gland, generally Occurs late in the patients with widespread systemic disease. Eyelid involvement and tissue necrosis. mixed cellularity type. diagnostic, binucleate Reed- Sternberg cell
- 36. T-CELL LYMPHOMA Rare Usually occurs during the late stage of systemic disease ,or As a manifestation of mycosis fungoides. Only one case of primary t-cell lymphoma in the orbit has been described.
- 37. (a) T-cell lymphoma limited to the eyelid with ulceration. (b) The histopathologic features include the Pautrier-like microabscess (a and b) Courtesy of Seymour Brownstein, MD.
- 39. Subtypes of Intra ocular involvement Primary Central Nervous System Lymphoma (PCNSL) Primary Uveal Lymphoma Metastatic Uveal Lymphoma Secondary Uveal Lymphoma Hodgkin’s Lymphoma.
- 40. PRIMARY INTRAOCULAR LYMPHOMA Primary vitreoretinal lymphoma Vitreous cells and Geographical subretinal pigment epithelial infiltrative masses. Independent nonmetastatic foci of pcnsl Primary uveal lymphoma Diffuse or multifocal creamy yellow choroidal infiltrates in one or both eyes. Associated with independent foci of visceral NHL
- 41. 06/14/15 Primary CNS Lymphoma (PCNSL) A subset of diffuse large B-cell NHL Increasing incidence and high mortality Usually affects elderly and is unilateral or bilateral Infiltrates the retina, vitreous, or optic nerve head 60-80% cases develop CNS disease Often masquerades as a chronic uveitis Typical clinical findings: vitritis and sub-RPE yellow–creamy infiltrates
- 42. Tumor cells in the anterior chamber ~75% of patients. Cells simulate iridocyclitis and form a pseudohypopyon. 20 anterior segment changes : Neovascularization of the iris Neovascularization of the iridocorneal angle Possible glaucoma. In rare circumstances, PCNSLO can form a mass in the iris or angle. 06/14/15
- 43. Primary vitreoretinal lymphoma. Typical geographical subretinal pigment epithelial lesion with relatively few vitreous cells.
- 44. Posterior segment : vitreous cells are a typical finding Fundus :low-lying, yellow-to-white mass deep to the sensory retina. Single or multiple, confluent or discrete. May appear as multiple punctate lesions. Infiltrative and involve all layers of the retina. PCNSLO : increased frequency in immunosuppressed 06/14/15
- 45. Classical pathological findings: atypical lymphoid cells between the RPE and Bruch's membrane, with monoclonality demonstrating IgH (for B-cell) orTCR (forT-cell) gene rearrangement Cytokines: elevation of IL-10 levels in the vitreous (for B-cell PIOL 06/14/15
- 46. Gross photograph of enucleated globe with PCNSL, revealing retinal thickening, hemorrhage, and RPE involvement large neoplastic cells with necrosis Vitreous cytology showing large neoplastic cells
- 47. Retinal hemorrhage is rarely seen. Deep infiltrates can give rise to exudative retinal detachment. If chorioretinal lesions regress, scarring and atrophy of the retinal pigment epithelium may be the only remaining fundus findings. Optic neuropathy may also be a feature 06/14/15
- 48. PCNSL involving vitreous and subretinal space Fluorescein angiogram of left eye during laminar flow phase, revealing early hypofluorescence of lesions noted in A. Fluorescein angiogram of same eye after 6 minutes, revealing intense staining of infiltrates.
- 49. Primary uveal lymphoma. Diffuse, creamy uveal infiltration with focal nodular accentuation inferotemporal to macula.
- 50. DIFFERENTIAL DIAGNOSIS PRIMARY VITREORETINAL LYMPHOMA PRIMARY UVEAL LYMPHOMA Chronic IdiopathicVitritis Vitiliginous Choroiditis Vitreous Amyloidosis Metastatic Carcinoma Cytomegalovirus Retinitis. Pars Planitis (Intermediate Uveitis) Leukemic Intraocular Infiltration Metastatic carcinoma Pneumocystis carinii choroiditis Benign reactive lymphoid Hyperplasia Posterior scleritis , Harada’s disease Bilateral diffuse uveal melanocytic proliferation associated with systemic carcinoma
- 51. Metastatic systemic lymphoma Confined to the uvea (esp: the choroid). Compared with PCNSLO, metastatic systemic lymphomas are much less prevalent have a better prognosis less likely to create a diagnostic dilemma. 06/14/15
- 52. 06/14/15 Diagnosis High index of suspicion Radiologic imaging Histologic analysis Vitreous biopsy Flow cytometry Subretinal aspiration Retinal biopsy
- 53. 06/14/15 Laboratory studies Complete blood count (CBC) with differential Serum immunoprotein electrophoresis Rapid plasma reagin (RPR) screening Erythrocyte sedimentation rate (ESR) Fluorescent treponemal antibody absorption (fta-abs) test Toxoplasma titers . Antinuclear antibodies (ANA) test Rheumatoid factor Angiotensin-converting enzyme (ACE) Cytomegalovirus (CMV) titers A tuberculosis skin test is advisable. The serum lactate dehydrogenase (LDH) Enzyme-linked immunosorbent assay (ELISA) for HIV is also recommended
- 54. 06/14/15 B-scan ultrasonography intraocular mass. retinal detachment. CT and MRI: low sensitivity for intraocular lymphoma do not facilitate differentiating the diagnosis against uveitis or ocular melanoma Imaging of the CNS with contrast to look for lesions elsewhere.
- 55. 06/14/15 Lumbar puncture : if CNS lymphoma is suspected. Bone marrow aspiration for staging systemic lymphomas. CT scans of the chest and abdomen to rule out retroperitoneal lymphoma. Bone scans may also be done Vitreous biopsy Retinal biopsy Orbital biopsy
- 56. 06/14/15 Because of the fragility of neoplastic lymphocytes, a specimen may contain numerous abnormal-appearing but uninterruptable cells. Molecular analysis : adjuncts to cytology for establishing the diagnosis of PCNSLO. immunoglobulin gene rearrangements and ocular cytokine levels elevated interleukin (IL)–10 IL-10–to–IL-6 ratio greater than 1.0, are helpful CDR3 polymorphism analysis to confirm clonality.
- 57. DIAGNOSIS OF LYMPHOMA CT helps in localizing orbital involvement Biopsy can provide the definitive diagnosis. Histopathology - cornerstone of the diagnostic process. Molecular pathology -to detect monoclonal gene Cytogenetic abnormalities such as chromosomal translocations or karyotypic abnormalities
- 58. 06/14/15 Treatment Radiotherapy RT + chemotherapy in the presence of central nervous system involvement. For non-Hodgkin's lymphoma, chemotherapy involves the use of iv Cyclophosphamide 750mg/m2 on days 1 and 8, iv Adriamycin 45mg/m2 on days 1 and 8, ivVincristine 1.5mg/m2 on days 1 and 8 and oral Prednisolone 20mg 8 hourly for 10days.
- 59. 06/14/15 For Hodgkin's lymphoma, chemotherapy involves the use ofABVD regimen iv Adriamycin 25mg/m2 on days 1and15; iv Bleomycin 10U/m2 on days 1and15; ivVinblastine 6mg/m2 on days 1and15 and iv Dacarbazine 375mg/m2 on days 1and15). High dose methotrexate and Leucovorin rescue may also be used for ocular lymphoma.
- 60. Multimodality therapy Boosted radiation dose (5000-10,000 cGy) to the spinal cord and Intrathecal methotrexate, Vision can be improved and life can be prolonged, with some patients alive at 9 years after treatment. 06/14/15
- 61. Multiagent primary chemotherapy Designed to reduce radiation-associated cognitive defects Can occur in up to 40% of patients older than 50 years. Methotrexate and procarbazine, vincristine, thiotepa, or both vincristine and cytarabine. Complete remission for long as 30 months 06/14/15
- 62. Lymphoid tumors of the conjunctiva Traditionally treated with local radiation therapy. Cryotherapy suggested Fewer ocular and systemic complications and lower cost 06/14/15
- 63. Primary orbital lymphoma Radiotherapy alone is highly effective Bilateral orbital disease with no systemic disease, is not an indication for chemotherapy. High-grade tumors may require up to 4000 cGy. shielding of the globe (lens-sparing technique) is to minimize ocular complications 06/14/15
- 64. , In some cases, combining such systemic therapy with local radiation treatment is beneficial. After radiotherapy, local control was achieved in 97-100% of patients. 06/14/15
- 65. Monoclonal antibody (mAb) Lymphomas respond well to mAb therapy, Rituximab, Ibritumomab Epratuzumab IV rituximab –for low-grade lymphoma showed good results. Antiangiogenic drugs – use of thalidomide is in study 06/14/15
- 66. References Albert & Jakobiec's principles & practice of ophthalmology Yanoff & Duker: ophthalmology, 3rd ed.2008,ch 8.4 Robbins and Cotran Pathologic Basis of Disease 7th ed 2005, pg 667 - 690 JAMA ophthalmol.Doi:10.1001/jamaophthalmol.2014.4644 published online november 13, 2014. JAMA ophthalmol.Doi:10.1001/jamaophthalmol.2014.376 published online april 24, 2014 AAOTextbook of Ophthalmic Pathology & Intraocular tumors.2011-2012, pg 323-326 06/14/15
- 67. THANK YOU