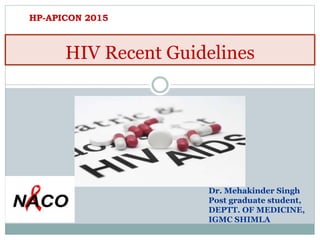
![Total: 35.0 million
[33.2 million – 37.2 million]
Middle East & North
Africa
230 000
Sub-Saharan Africa
24.7 million
Eastern Europe &
Central Asia
1.1 million
Asia and the Pacific
4.8 million
North America and Western and Central
Europe
2.3 million
Latin America
1.6 million
Caribbean
250 000
Adults and Children
Estimated to be living with HIV2013
Since the beginning of the pandemic an estimated
39 million people have died of AIDS related illnesses](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to Hiv recent guidelines naco 2015
Similar to Hiv recent guidelines naco 2015 (20)
More from Mehakinder Singh
Recently uploaded
Recently uploaded (20)
Hiv recent guidelines naco 2015
- 1. HIV Recent Guidelines Dr. Mehakinder Singh Post graduate student, DEPTT. OF MEDICINE, IGMC SHIMLA HP-APICON 2015
- 2. Total: 35.0 million [33.2 million – 37.2 million] Middle East & North Africa 230 000 Sub-Saharan Africa 24.7 million Eastern Europe & Central Asia 1.1 million Asia and the Pacific 4.8 million North America and Western and Central Europe 2.3 million Latin America 1.6 million Caribbean 250 000 Adults and Children Estimated to be living with HIV2013 Since the beginning of the pandemic an estimated 39 million people have died of AIDS related illnesses
- 3. Estimates for Adults and Children in India Estimated People living with HIV 2,100,000 Adults aged 15 to 49 prevalence rate 0.27% Adults aged 15 and up living with HIV 1,900,000 Women aged 15 and up living with HIV 750,000 Deaths due to AIDS 140,000 Source: UNAIDS Global Report 2013; NACO HIV Estimations 2012
- 4. • On the basis of the HIV Technical report on HIV estimates-2012 the epidemic of HIV /AIDS in Himachal Pradesh is static and under control. • Our state fall under the low prevalence category where the infection rate among the adult HIV prevalence is 0.17%. • There are 8091 confirmed HIV positive persons in the State till March 2015. HIV/AIDS Situation in H.P. 4
- 5. National response to HIV/AIDS in India 1986: First case of HIV detected in Chennai 1990: HIV/AIDS Cell set up in MoHFW 1992: National AIDS Control Organisation (NACO) established within MoHFW 1994-1999: NACP-I launched with a budget of Rs. 468.4 crores 1999-2006: NACP-II Budgetary Support: Rs. 2,690 crores 2007-2012: NACP-III Budgetary Support: Rs. 8,023 crores 2012-2017: NACP-IV Budgetary support: Rs.14,295 crores
- 6. 57% Reduction in New Infections (2001-12) with Scale-up of Prevention Strategies 29% Reduction in AIDS-related Deaths (2006-12) with Scale-up of Anti-Retroviral Treatment Source: UNAIDS Global Report 2013; NACO HIV Estimations 2012 Evidence of Programme Impact in India AIDS related deathsNew Infections
- 7. HIV Care in General Health System 26 Link ART Centres and LAC Plus Centres (987) ART Centres (448) CoE & ART Plus Centres( 54) Three-Tier Model of HIV Treatment ServicePublic Health Infrastructure Selected Medical Colleges Medical colleges and District Level Hospitals Sub-District level Hospitals & CHC Updated September 2014 CoE 10 PCoE 7 ART plus 37 Total CST Facilities: 1435
- 8. Diagnosis of HIV Infection National Guidelines on Testing Adults • For symptomatic persons: the sample should be reactive with two different kits • For asymptomatic persons: the sample should be reactive with three different kits
- 9. Diagnosis of HIV Infection
- 10. Pre – ART Care and Follow up At the beginning of HIV care and prior to starting ART, a clinical assessment should be performed to: Determine the clinical stage of HIV infection Identify history of past illnesses (especially those related to HIV) Identify current HIV-related illnesses that require treatment Determine the need for ART and OI prophylaxis Identify coexisting medical conditions and treatments that may influence the choice of therapy 10
- 13. 13
- 15. Primary OI Prophylaxis for adult Opportunistic Infection Choice of Antimicro bial Indication Discontinue, if CD4 counts stable for > 6 months PCP CTX – DS, 1 tab OD <250 cells/cmm >250 cells/cmm Toxoplasmosis CTX – DS, 1 tab OD <250 cells/cmm >250 cells/cmm Cryptococcal Meningitis - Not recommended - Mycobacterium TB - Not recommended - MAC - Not recommended - Candidiasis - Not recommended - CMV Retinitis - Not recommended - Primary Prophylaxis
- 16. Upto October 2014: Cotrimoxazole Prophylaxis When and How to initiate Cotrimoxazole Prophylaxis Commencing primary CPT WHO clinical stage I and II: CD4 <250 cells/mm3 or WHO clinical stage III and IV: Irrespective of CD4 count Commencing secondary CPT For all patients who have completed successful treatment for PCP until CD4 is >250 maintained over a period of 6 months Timing the initiation of cotrimoxazole in relation to initiating ART Start cotrimoxazole prophylaxis first. Start ART about two weeks later if the patient can tolerate cotrimoxazole and has no symptoms of allergy (rash, hepatotoxicity) Meanwhile, make use of the time for adherence and treatment preparation Dosage of cotrimoxazole in adults & adolescents One double-strength tablet or two single-strength tablets once daily – total daily dose of 960 mg (800 mg SMZ + 160 mg TMP)
- 17. Revised guidelines on Timing of ART initiation in relation cotrimoxazole prophylaxis (November 2014 Guidelines) The existing guidelines stipulate that there shall be two weeks of cotrimoxazole administration before initiating first line ART. “Start ART about two weeks later if the patient can tolerate cotrimoxazole and has no symptoms of allergy (rash, hepatotoxicity)” However keeping in mind that many patients are lost in this period if not initiated on ART and also keeping in mind benefits of early ART initiation, especially in those with low CD 4 count, it has been decided that ART should be started 5-6 days after start of CPT prophylaxis or as soon as CPT is tolerated and patients has completed the “preparedness phase "of counselling 17
- 18. Do not start ART in the presence of an active OI. In general, OIs should be treated or stabilized before commencing ART. 18
- 19. Antiretroviral Therapy (ART) ART is the combination of different classes of ARV drugs To achieve maximal and most durable suppression of viral replication To prevent emergence of drug resistant mutants To improve survival and quality of life Before ART One year after ART
- 20. HIV Lifecycle
- 21. Mechanism of Anti Retro Viral Drugs Action 4 Fusion Inhibitor Enfuviritide CCR5 co receptor Antagonist Maraviroc NRTIs NNRTIs Integrase Inhibitors Protease Inhibitors NsRTI Nevirapine (NVP) Efavirenz (EFV) Etravirine Rilpivirine Delavirdine, DLV Raltegravir RGV Elvitegravir ELV Dolutegravir DTG Atazanavir (ATV) Ritonavir (RTV) Lopinavir (LPV) Saquinavir (SQV) Indinavir (IDV) Nelfinavir (NFV) Amprenavir (APV) Fosamprenavir, (FPV) Tipranavir (TPV) Darunavir (DRV) Zidovudine (AZT) Stavudine (d4T) Lamivudine (3TC) Abacavir (ABC) Didanosine (ddI) Emtricitabine (FTC) NtRTI Tenofovir (TDF)
- 22. Initiation of ART based on CD4 count & WHO Clinical staging WHO Clinical Staging Recommendations HIV infected Adults & Adolescents Clinical Stage I and II Start ART if CD4 <350 cells/mm3 Clinical Stage III and IV Start ART regardless of CD4 count For HIV and Hepatitis B and C co-infected patients HIV and HBV / HCV co-infection - Without documented evidence of severe chronic liver disease Start ART if CD4 <350 cells/mm3 HIV and HBV / HCV co-infection - With documented evidence of severe chronic liver disease Start ART regardless of CD4 count
- 23. Evolution of WHO ART Guidelines TOPIC 2002 2003 2006 2010 When to start ART CD4 ≤200 CD4 ≤ 200 CD4 ≤ 200 - Consider 350 - CD4 ≤ 350 for TB CD4 ≤ 350 -Irrespective CD4 for TB & HBV PMTCT Since 2001 4 weeks AZT; AZT+ 3TC, or single dose NVP 2004 AZT from 28 weeks + single dose NVP AZT from 28 weeks + single dose NVP +AZT/3TC 7days Option A (AZT +infant NVP) Option B (triple ARVs) First line ART 8 options - AZT preferred 4 options - AZT preferred 8 options - AZT or TDF preferred - d4T dose reduction 6 options & FDCs - AZT or TDF preferred - d4T phase out Second line ART Boosted PI Boosted PI Boosted PI ATV/r, DRV/r, FPV/r LPV/r, SQV/r Boosted PI Heat stable FDC: LPV/r, ATV/r Viral load Testing No No (Desirable) Yes Tertiary centres Yes Phase in Earlier initiation Simpler treatment Safer, more robust regimens Better monitoring Simplified treatment options for pregnant women Vitoria M et al, Curr Opin HIV/AIDS 2013
- 24. National ART Regimens Summary of Changes in WHO Recommendations When to Start in Adults Target population (ARV-Naive) 2010 ART Guidelines 2013 ART guidelines Strength of Recommendation & Quality of Evidence HIV+ Asymptomatic CD4 ≤350 cells/mm3 CD4 ≤500 cells/mm3 (CD4 ≤350 cells/mm3 as a priority) Strong, recommendation moderate-quality evidence HIV+ Symptomatic WHO clinical stage 3 or 4 regardless of CD4 cell count No change Strong, moderate- quality evidence Pregnant and breastfeeding women with HIV CD4 ≤350 cells/mm3 or WHO clinical stage 3 or 4 Regardless of CD4 cell count or WHO clinical stage Strong, moderate- quality evidence HIV-TB co-infection Presence of active TB disease, regardless of CD4 cell count No change Strong, low-quality evidence HIV-HBV CO-INFECTION Evidence of chronic active HCV disease, regardless of CD4 cell count Evidence of severe chronic HBV liver disease, regardless of CD4 cell count Strong, low-quality evidence HIV+ Partners in Sero discordant Couple No recommendation established Regardless of CD4 cell count or WHO clinical stage Strong, high-quality evidence
- 25. WHO 30th September 2015
- 27. Summary of Changes in Recommendations: on What to Start in Adults First-line ARV regimens Target population 2012 ART Guidelines 2014 ART Guidelines HIV+ adults AZT or TDF + 3TC + EFV or NVP TDF + 3TC + EFV (as fixed dose combination) HIV+ pregnant women AZT + 3TC + NVP or EFV HIV-TB Co-infection AZT or TDF + 3TC + EFV HIV-HBV / HBC Co-infection TDF + 3TC + EFV TARIKA 300mg LOVABLE 300mg EXPERIENCE 600mg
- 28. 28
- 29. In India, the agreed practical definition of IRIS would be the “occurrence or manifestations of new OIs or existing OIs within six weeks to six months after initiating ART; with an increase in CD4 count”. IRIS (NACO May 2013)
- 30. Most commonly present with fever and worsening of pre-existing lymphadenopathy or respiratory disease. There are no standard guidelines for the treatment of IRIS. Most cases resolve without any additional treatment. Milder forms of IRIS resolve with continuing anti-infective therapy and HAART. In the majority of cases, HAART can be safely continued and need not be interrupted. IRIS
- 31. However, the discontinuation of ART should be considered if the inflammatory responses are considered life-threatening (e.g. intracranial IRIS leading to encephalitis, cerebritis, perilesional cerebral oedema and pulmonary IRIS with ARDS/acute respiratory distress syndrome), or are unresponsive to steroids. Non-steroidal anti-inflammatory drugs (NSAIDs) are helpful in controlling inflammation and fever associated with IRIS. However, in severe IRIS, a short course of oral prednisolone is required to alleviate the symptoms. IRIS
- 32. First line ART: Drug Toxicities Drugs Short term toxicities Medium term toxicities Long term toxicities Zidovudine Headache, nausea, vomiting, malaise, Diarrhoea Bone Marrow suppression Anaemia (Macrocytic) Bone Marrow suppression Anaemia (Macrocytic) Hyper pigmentation Lactic Acidosis Proximal myopathy Stavudine Lactic Acidosis Pancreatitis Peripheral Neuritis Lipodystrophy Dyslipidemia Tenofovir Nephrotoxicity (low incidence), Fanconi syndrome and rarely Acute Renal Failure Nevirapine Skin Rashes Hepato toxicity Efavirenz Drowsiness, dizziness, Confusion, Vivid dreams Skin Rashes Hepato toxicity (very rare)
- 33. Drug Substitution Drug Toxicity Drug Substitution Zidovudine Persistent GI intolerance or severe haematological toxicity Substitute with Tenofovir Tenofovir Nephrotoxicity Fanconi syndrome Acute Renal Failure Substitute with Zidovudine, if Hb is >9 gm/dl Substitute with Stavudine, if anaemic (Hb is <9 gm/dl) Both Zidovudine and Tenofovir As above Substitute with Stavudine
- 34. Drug Substitution Drug Toxicity Drug Substitution Nevirapine Hepatotoxicity, Skin rash but not life threatening (Except Grade 4) Substitute with Efavirenz Severe rash; life threatening (Grade 4): Stevens-Johnson syndrome to Nevirapine Substitute with Atazanavir/ritonavir Efavirenz Persistent CNS toxicity Substitute with Nevirapine Both Nevirapine and Efavirenz As above Substitute with Atazanavir/ritonavir
- 35. Efavirenz: CNS Effects • CNS toxicity: Vivid dreams, nightmare, insomnia, dizziness, headache, impaired concentration and attention span, depression, hallucination, exacerbation of psychiatric disorders, psychosis and suicidal ideation • CNS effects (at least some) are observed during first few doses of Efavirenz in >50% of patients – Typically starts after 1st and / or 2nd dose of Efavirenz – Usually subsides by 2 to 6 weeks 35
- 37. Refer to SACEP Suspect treatment failure during the medical consultation • Clinical: Advancing T-stage of disease – WHO stage 3/4 conditions • Fall of CD4 count to pre-therapy baseline • 50% fall from the on-treatment peak value • Persistent CD4 levels below 100 cells Signs or symptoms of OI Manage IRIS or OI, especially TB Repeat CD4 immediately Perform clinical staging Give prophylaxis and/or treatment for OI Continue 1st line ART and support adherence Work with patient / caregiver to resolve issues causing non-adherence Continue First line ART, give OI prophylaxis if necessary Follow-up monthly; Reassess clinically Repeat CD4 after two weeks (to confirm validity and exclude lab and physiological variability) If CD4 not declining, continue adherence support and repeat CD4 in 3 months. Reassess and determine if treatment failure NOPatient has been on ART for at least 6 months Is adherence to first-line ART optimal? YES YES Most recent CD4 within 1 month of current medical consultation CD4 indicating treatment failure? YES YES NO NO NO State AIDS Clinical Expert Panel 37
- 38. Current Recommendation for Second line ART is based on: A new class of ARV, a Ritonavir boosted PI (Atazanavir/ritonavir or Lopinavir/ritonavir) Supported by at least one new and unused NRTI (Zidovudine or Tenofovir or Stavudine) Continued Lamivudine administration ensures reduced viral fitness Formulation of Second line ART
- 39. For PLHIV failed to Tenofovir based First line ART Regimens Regimen ART Regimen Preference Regimen III Zidovudine + Lamivudine + Atazanavir/ritonavir Second line regimen for those who were on Tenofovir containing first line regimen, if Hb >9gm/dl Regimen III(a) Zidovudine + Lamivudine + Lopinavir/ritonavir For patients of Regimen III, who developed severe Atazanavir toxicity Regimen V Stavudine + Lamivudine + Atazanavir/ritonavir Second line regimen for those who were on Tenofovir containing first line regimen, if Hb <9gm/dl Regimen V(a) Stavudine + Lamivudine + Lopinavir/ritonavir For patients of Regimen V, who developed severe Atazanavir toxicity
- 40. ART IN SPECIAL SITUATIONS
- 41. ART Regimen Indications Tenofovir 300mg + Lamivudine 300 mg + Lopinavir/ritonavir (800/200) First line regimen for patients with confirmed HIV-2 infection alone or combined HIV-1 and HIV-2 infection, regardless of Hb level HIV-2 Infection: NACO ART Regimen 41
- 42. Paediatric HIV can be prevented by effective PPTCT 42
- 43. NACO Guidelines (December 2013) What ART to Start in Pregnant & Breast-feeding Women Life long therapy Tenofovir + Lamivudine + Efavirenz for all HIV Positive Pregnant and breast feeding women regardless of clinical stage or CD4 count or duration of pregnancy <Rolled out across the country from January 2014>
- 44. HIV-positive partners in HIV sero-discordant couples The results of the HPTN052 study strongly support the use of ART to prevent HIV transmission among HIV-sero-discordant couples (96% reduction) The Guidelines, therefore, endorse that the sexual partner with HIV in a sero-discordant couple should be offered ART regardless of CD4 count
- 45. Considerations for Co-infection of Tuberculosis and HIV HIV-TB co-infection is one of the most challenging issues in the effort to scale up ART since more than 60% of PLHIV develop TB. Active TB is the commonest OI among HIV- infected individuals and is also the leading cause of death in PLHIV.
- 46. Initiation of First line ART in PLHIV with TB Co-infection Type of Tuberculosis Eligible Clinical Staging and CD4 Counts Timing of ART in relation to start of TB treatment ART Regimen Pulmonary TB (Stage III) Start ART irrespective of any clinical stage and irrespective of any CD4 count Start ATT first (Category I or II) Start ART as soon as TB treatment is tolerated (after 2 weeks & before 2 months) TDF+3TC+EFV (Single pill at bed time)Extra pulmonary TB (Stage IV)
- 47. Second Line ART for HIV-TB in India Tenofovir / Zidovudine / Stavudine + Lamivudine + Atazanavir/ritonavir 47
- 48. Management Plan for TB in patients on Second line ART & Alternate First line ART (Receiving Atazanavir/ritonavir or Lopinavir/ritonavir) Rifampicin suppresses the action of boosted PI (Atazanavir/ritonavir or Lopinavir/ritonavir) However, Rifabutin does not suppress the action of Atazanavir/ritonavir or Lopinavir/ritonavir Ritonavir boosts Rifabutin availability Rifabutin 300 mg thrice weekly has to be substituted for Rifampicin in category I or II treatment protocol 48
- 50. HIV negative HIV Source code No PEP required Status/Source unknown HIV SC unknown HIV positive Low titer exposure Asymptomatic, high CD4 High titer exposure Advanced disease, low CD4 HIV SC1 HIV SC2 HIV status of exposure source
- 51. No Is the Source material is blood, bloody fluid or Other Potentially Infected Material (OPIM) or an instrument contaminated with one of these substances? Mucous Membrane or Skin integrity compromised Volume Small volume- few drops / short duration Large volume- major splash / long duration Less severe- solid needle, Superficial scratch No PEP required Intact Skin only No PEP required Severity EC 2 EC 3EC1 EC 2 What Type of exposure has occurred? More severe- hollow bore, deep injury Percutaneous exposure Yes HIV Exposure code 51
- 52. Revised PEP Recommendations {December, 2014} Occupational Exposure Exposure Code HIV Source Code PEP Recommendations Duration 1 1 Not warranted 28 days 1 2 Recommended 2 1 2 2 3 1 or 2 2/3 Unknown Consider PEP, if HIV prevalence is high in the given population & risk categorisation
- 53. PEP Regimens Revised Guidelines - December, 2014 a. Wherever PEP is indicated and source is ART naive or unknown: recommended regimen is Tenofovir 300 mg + Lamivudine 300 mg + Efavirenz 600 mg once daily for 28 days. • Wherever available, single pill containing these formulations should be used. • Dual drug regimen should not be used any longer in any situation for PEP b. The first dose of PEP regular should be administered as soon as possible, preferably within 2 hours of exposure and the subsequently dose should be given at bed time with clear instruction to take it 2-3 hours after dinner & to avoid fatty food in dinner
- 54. In case of Sexual Assault: PEP should be provided to exposed person in case of sexual assault as a part of overall package of post sexual assault care Revised PEP Recommendations {December, 2014}
- 55. Pre- vs Postexposure Prophylaxis After exposure to HIV, infection may become established Postexposure prophylaxis (initiated soon after exposure) reduces the chance of infection Pre-exposure prophylaxis begins treatment earlier (before exposure), which might increase the prophylactic effect HIV infection 0 hr 36 hrs 72 hrs HIV exposure 1 mos 3 mos 5 mos Postexposure prophylaxis Pre-exposure prophylaxis 55
- 56. CDC Guideline: Recommended PrEP Regimen Fixed-dose TDF/FTC is the recommended PrEP regimen for MSM, heterosexually active men and women, and IDU who meet PrEP prescribing criteria Dosed as a single pill (300/200 mg) once daily This regimen is approved by the FDA for PrEP use Provide a prescription or refill for no more than 90 days TDF alone may be considered as an alternative for IDU and heterosexually active men and women (but not MSM) Based on efficacy data from clinical trials This regimen is NOT approved by the FDA for PrEP use
- 57. Palliative Care in HIV The Government of India has adopted WHO’s definition of palliative care, which is the active total care of patients whose disease is not responsive to curative treatment (Manual on Palliative Care, MOHFW, November 2005).
- 58. End-of-life Care “ How people die lives on the memory of those left behind” The terminal phase is defined as the period when day-to- day deterioration, particularly of strength, appetite and awareness are occurring. The aim of care at this stage should be to ensure the patient’s comfort holistically, and a peaceful and dignified death. Provide psychosocial and spiritual support to the patient. Help the family come to terms with the fact that the patient is leaving them soon: let family members be around to see and talk to the patient 58
- 59. ART PLUS CENTRE Shimla <September 2015> Total PLHIV registered- 2392 Started on ART- 1553 (alive 482, dead 310, LFU 56, optout 15, transfer out 689, stopped 1) PLHIV on 2nd line ART – 7 Pre ART – 839 (alive 77, dead 154, LFU 278, opt out 18, transfer out 312)
- 60. G U R U N A N A K “In the places where the lowly and discarded are cared for, there resides the blessings of Your Grace” Thank you
- 66. Cotrimoxazole Prophylaxis When to stop Cotrimoxazole Prophylaxis When to stop prophylaxis (cotrimoxazole or dapsone) in patients on ART If CD4 count >250 for at least 6 months and If patient is on ART for at least 6 months, is asymptomatic and well Cotrimoxazole for pregnant women- Women who fulfill the criteria for CPT should be started on and continued on it throughout pregnancy. Breastfeeding women should continue CPT where indicated Patients allergic to sulpha-based medications should be given Dapsone 100 mg per day, if available
- 67. Do not start ART in the presence of an active OI. In general, OIs should be treated or stabilized before commencing ART. Mycobacterium Avium Complex (MAC) and progressive multifocal leukoencephalopathy (PML) are exceptions, in which commencing ART may be the preferred treatment, especially when specific MAC therapy is not available. 23
- 68. HIV status of source of exposure Source of HIV Definition of Risk in Source HIV Negative Source is not HIV infected; but consider HBV & HCV Low Risk HIV Positive and clinically Asymptomatic High Risk HIV Positive and clinically Symptomatic Unknown • Status of the patient unknown • Neither patient nor his / her blood available for testing • The risk assessment will be based only upon the exposure (HIV Prevalence in the geographical area should be considered)
- 69. 8 National ART Regimens NACO ART Regimen Revised 2012 Regimen National ART Regimen Indications & Comments Regimen I Zidovudine + Lamivudine + Nevirapine First line regimen for patients with Hb >9 gm/dl Regimen I (a) Tenofovir + Lamivudine + Nevirapine First line regimen for patients with Hb <9 gm/dl Regimen II Zidovudine + Lamivudine + Efavirenz First line regimen for patients with Hb >9 gm/dl and on concomitant Rifampicin containing ATT Regimen II (a) Tenofovir + Lamivudine + Efavirenz • First line regimen for patients with Hb <9 gm/dl and on concomitant Rifampicin containing ATT • First line regimen for all patients with Hepatitis B & Hepatitis C co- infection • First line regimen for pregnant women, with no exposure to sd- NVP / NNRTI in the past
- 70. ART Regimen for those already “on ART” Regimen Already on ART Regimen ART Continuation Drug Dispensing Regimen I Zidovudine + Lamivudine + Nevirapine Continue Zidovudine + Lamivudine + Nevirapine Regimen I (a) Tenofovir + Lamivudine + Nevirapine Tenofovir + Lamivudine + Efavirenz (Single Pill) Regimen II Zidovudine + Lamivudine + Efavirenz Continue Zidovudine + Lamivudine + Efavirenz (ZLE) even after ATT is completed , if on ATT Regimen II (a) Tenofovir + Lamivudine + Efavirenz Tenofovir + Lamivudine + Efavirenz (Single Pill)