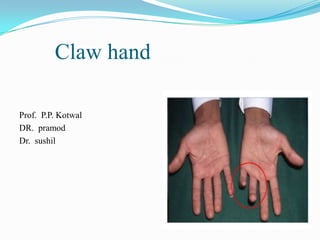
2. Definition
Flattening of transverse
metacarpal arch and
longitudinal arches, with
hyperextension of MCP
joints and flexion of PIP
and DIP joints
3. Normal anatomy
Movements of MP joints and IP joints independent
Movements of 2 IP joints coordinated ; flexion of DIP
joint brings about flexion of PIP joint
(1) Flexion of distal phalanx draws dorsal expansion
distally by loosening tension on central tendon
(2) Flexion of DIP joint tenses oblique retinacular
ligament causing this ligament to slide volarward and
impart flexion force to PIP joint
Landsmeer JMF: The coordination of finger-joint motions. J Bone Joint Surg Am 1963
7. Patho-anatomy of deformity
Paralysis of interossei and lumbricals
Unopposed MCP joint extension & IP joint flexion by
digital extensors & flexors
Without stabilization of MCP joints in neutral/slight
flexed position, long extensor function “blocked” at
MP joint by diversion of this tension to sagittal band,
producing hyperextension and effectively blocking the
extensor's ability to extend PIP joint.‡
‡Mulder JD, Landsmeer JMF: The mechanism of claw finger. J Bone Joint
Surg Br 1968
8.
9. Middle and distal phalanges collapse into flexion
Normal cascade of digital extension disrupted, in that
during any attempt to actively open finger, MP joint
extends first and will extend more than the PIP joint,
Normal sequence of digital closure also reversed, in
that IP joint flexion precedes MP joint flexion
Independence of MP and IP joint motion lost
11. Claw thumb in Ulnar palsy
CMC joint affected by paralysis of adductor pollicis,
FPB, and first dorsal interosseous
MP and IP joints of thumb under control of extrinsic
flexors and extensors, with proximal phalanx behaving like
intercalated bone.
MP joint will go into hyperextension and IP joint into
flexion because of the greater extensor moment at the MP
joint and the lesser extensor moment at the IP joint,
respectively.
“Z”-thumb deformity
Brand PW, Hollister A: Mechanics of individual muscles at individual joints. Clinical Mechanics of the
Hand, 2nd ed.. St. Louis: Mosby–Year Book; 1993
12. Types of claw hand
Complete : Involving all digits and resulting from
combined Ulnar and Median Nerve palsy
Incomplete : Involving only ulnar 2 digits as in
isolated Ulnar Nerve palsy
13. Partial Claw hand
Flexion Extension Deformity
MCP Joint Lumbricals Extensor Hyper extension of
paralyzed Digitorum active MCP jOINT
PIP Joint FDS active Interossei Flexion of PIP
paralyzed ( low joint
Ulnar palsy )
DIP Joint FDP active Interossei Flexion of DIP
paralyzed
FDP paralyzed( Interossei Neutral position
high Ulnar Palsy ) paralyzed
14. Total Claw Hand
Flexion Extension Deformity
MCP Joint Lumbricals Extensor Hyper extension at
paralyzed digitorum active MCP
PIP Joint FDS paralyzed Extensor Extension of PIP
digitorum active
DIP Joint FDP paralyzed Extensor Extension of DIP
digitorum active
17. Pattern of Injury
Low mixed Ulnar and median nerve palsy
High mixed Ulnar and Median nerve palsy
Low Ulnar nerve palsy
High Ulnar nerve palsy
20. Specific signs and tests for motor dysfunction
Duchenne's sign : Hyperextension at MCP joints &
flexion at IP joints
Bouvier’s maneuver : Dorsal pressure over proximal
phalanx to passively flex MP joint results in
straightening of distal joints and temporary
correction of claw deformity
Extensor digitorum tendon can extend middle and
distal phalanges when proximal phalanx stabilized
Andre-Thomas sign : On palmar -flexon of wrist
exaggeration of deformity
21. Pitres-Testut sign : Inability to actively move long
finger s in radial and ulnar deviation with palm placed
flat
Cross your fingers test : Inability to cross middle
finger dorsally over index finger, or index over
middle finger
Masse's sign: Flattened metacarpal arch and loss of
hypothenar elevation
Wartenberg's sign : Inability to adduct extended
little finger to extended ring finger
22. Jeanne’s sign : Hyperextension of MP joint of thumb
during key pinch or gross grip
Froment’s sign : Thumb IP joint flexion while
attempting to perform lateral pinch
Bunnell’s O sign : Combined hyperextension at MP
joint and hyperflexion of IP joint (noticed when
patient makes a pulp to pulp pinch with thumb and
index finger)
26. Pollock's sign : Inability to flex distal phalanges of
ring and little fingers
Partial loss of wrist flexion may occur because of
paralysis of FCU
Weakness of ulnar side grip
27. PREOPERATIVE ANGLE MEASUREMENTS
Measured at PIP joint of each finger and IP joint of thumb
using a goniometer placed on dorsal aspect of joint
Unassisted angle : Maintain “lumbrical-plus” position of
MP flexion and IP extension, and extension deficit at PIP
joint measured
Assisted angle : Proximal segment of finger supported to
maintain flexion at the MP joint and instructs the patient
to extend IP joints ;In absence of contracture of IP joints,
this angle o
28. Contracture angle : Incomplete passive extension
,contracture with deficiency of volar skin and volar plate
and/or capsule PIP joint
Adaptive shortening angle of extrinsic flexors :
Habitual posturing of wrist in flexion to minimize the claw
deformity ; increased angulation at PIP joint as wrist is
passively moved into extension
Hypermobile angle: Ligamentous laxity ; hypermobile
joints with passive hyperextension of PIP joints > 20
29. CLASSIFICATION OF PARALYTIC CLAW HANDS
Type I: Supple claw hands with no hypermobile joints
and no contractures at IP joints
Type II: Hypermobile joints; PIP joints hyperextension >
20 degrees
Type III: Mobile joints in association with adaptive
shortening of long flexors, usually superficialis tendons ,
with no IP joint contracture
Anderson GA: Analysis of paralytic claw finger correction using flexor motors into different
insertion sites. Master's thesis, University of Liverpool, 1988.
30. Type IV: Contracted claw hands ; PIP joint flexion
contracture of 15 degrees or more, due to volar skin,
joint capsule, or volar plate contracture ± adaptive
shortening of long flexors
Type V: Claw hands with attrition of dorsal extensor
apparatus at PIP joint with “hooding deformity,”
fibrous or bony ankylosis of PIP joint, and MP joint
extension contracture
31. Principle
Clawing principal longitudinal axial deformity and
loss of independence of movement at MP and PIP
joints principal disability
Third muscle-tendon unit needs to run volar to
center of curvature of MP joint and dorsal to center of
curvature of head of PIP joint to counterbalance
system and provide equilibrium and independence of
normally functioning intrinsic muscles
Alternatively, MP joint needs to be statically
prevented from hyperextension to allow long
extensors to extend IP joints
32. Indications for surgery
Nerve Injuries
Patient referred late ( 1 year )
After nerve repair, if electrodiagnostic tests show no
signs of reinnervation within 6 to 9 months
*Jobe MT, Wright PE: Peripheral nerve injuries. In: Canale ST, ed. Campbell's Operative
Orthopaedics, 4. 9th ed.. St. Louis: Mosby; 1992
33. Leprosy
Understanding of stage and activity of disease, presence of intact,
healthy skin, patient motivation.*
Recommended when
patient's medical treatment optimized
skin smears for the bacillus negative
bacteriological index negative on two successive tests
disease activity quiescent for at least a year before date of intended
surgery,
paralysis established
patient free of corticosteroid treatment for several months before
surgery
*Enna CD: Preoperative evaluation. In: McDowell F, Enna CD, ed. Surgical rehabilitation in leprosy and in
other peripheral nerve disorders, Baltimore: Williams & Wilkins; 1974
34. Poliomyelitis
Ulnar innervated lumbricals can be paralyzed, sparing a
part of or whole of interosseous muscles or vice versa
Paralysis typically nonprogressive and with no loss of
sensation
Children affected, and joints hypermobile
Surgery be delayed until child is at least 5 years of age, so
that child will be able to cooperate with postoperative re-
education program
Anderson GA: The child's hand in the developing world. In: Gupta A, Kay SPJ, Scheker LR, ed. The Growing Hand:
Diagnosis and Management of the Upper Extremity in Children, London: Mosby; 2000
35. Appropriate use of splints, fabricated for each patient
and altered or changed whenever indicated can help to
manage claw deformity
Splints interfere with rehabilitation of sensibility and
are generally used intermittently
North ER, Littler JW: Transferring the flexor superficialis tendon:
Technical considerations in the prevention of proximal interphalangeal
joint disability. J Hand Surg [Am] 1980
36. Tendon transfers
Principles and biomechanics
Homeostasis of involved extremity established *
Soft tissues free of scar contracture
Vascularity of extremity adequate
Chronic wounds fully settled for 3 months before surgery
Proper physiotherapy, occupational therapy and splinting
Mobile joints and correct alignment of bone
Omer Jr GE: The technique and timing of tendon transfers. Orthop Clin North Am 1974
37. Power of transferred muscle : Good or normal (4 or 5)
Muscle should be expendable
Synergestic muscles
Path of Tendon: Best in straight line; If change in direction
necessary - Pulley
Absolute contraindication: Non-compliant patient
with poor motivation who will not follow appropriate
postop rehabilitation
38. Internal splints (Early Tendon Transfers)
Burkhalter
Allow early function of hand while awaiting nerve
regeneration
Can prevent deformities that lead to contractures
Improve coordination of residual muscle-tendon
units
Burkhalter WE: Early tendon transfers in upper extremity peripheral nerve injury. Clin Orthop 1974
39. Contd…
Stimulate sensory re-education during nerve recovery
Inhibition of trick movements
Functions as internal splints for paralyzed muscles
In the event of a failure of nerve recovery will remain
and function as a permanent solution
40. Contd…
Proximal phalanx flexion for ring and little
fingers : Ulnar half of FDSR with split insertion to
ring and little fingers to lateral band of DEE or A1, A2,
or A1 + A2a pulleys
Restoration of transverse metacarpal arch and
adduction of little finger : FDSR Y insertion
Thumb adduction for key pinch : FDSR radial half
to abductor tubercle, FDSL to hypothenar insertion,
near fifth MP joint
42. METHODS OF CLAW HAND RECONSTRUCTION
Static and Dynamic procedures
Static procedures :
To maintain MP joint in some degree of flexion or to
limit MP joint hyperextension
claw posture reversed by functioning long extensors
Flexion of MP joint unrestricted in static procedures
Disadvantages : restore normal finger coordination
and sequence but do not provide an additional motor to
restore MP flexion.
Recurrence : rule unless there is radical change in
patient's work style and paralyzed hand more protected
than used
43. Proximal Phalangeal Flexion Static Techniques
Flexor Pulley Advancement ( Bunnell )*
Each side of proximal pulley system split 1.5 to 2.5 cm up to
middle of the proximal phalanx.
Flexor tendons then “bow string,” to bring about flexion at
MP joint
Fasciodermadesis ( Zancolli )‡
Excision of 2 cm of the palmar skin (dermadesis) at MP joint
level combined with shortening of pretendinous band of palmar
aponeurosis (fasciodermadesis) to correct claw hands with weak
extensors
*Bunnell S: Surgery of the intrinsic muscles of the hand other than those producing opposition of
the thumb. J Bone Joint Surg 1942
‡Zancolli EA: Structural and Dynamic Bases of Hand Surgery, 2nd ed.. Philadelphia: JB Lippincott;
1979
44. Zancolli
Capsulodesis
Volar MP joint Capsulodesis
A1 pulley release with MP
joint volar plate advancement
Complicated claw hands with
MP joint contracture Zancolli
incorporated collateral ligament
release on both sides of MP joint
with volar capsuloplasty
Zancolli EA: Claw-hand caused by paralysis of the intrinsic muscles: A
simple surgical procedure for its correction. J Bone Joint Surg Am 1957
45. Omer advanced volar
plate by cutting away a
triangular portion of the
deep transverse
metacarpal ligament
(DTML) on each side of
volar plate flap
Omer Jr GE, Spinner M, ed.
Management of Peripheral
Nerve Problems,
Philadelphia: WB Saunders;
1980
46. Dorsal Methods (Howard; Mikhail)
To provide bony block to proximal phalangeal
extension
Enables long extensors to extend IP joints and correct
deformity.
Mikhail inserted bone block on dorsum of the
metacarpal head
Howard suggested elevation of bone wedge as block
from the dorsal aspect of the metacarpal head itself
Mikhail IK: Bone block operation for clawhand. Surg Gynecol Obstet 1964
47. Static Tenodesis Techniques
Riordan
One half of ECRL and ECU tendons made use of
as “grafts” to prevent hyperextension of MP joint while
remaining half continue to actively extend wrist
Riordan DC: Tendon transfers for nerve paralysis of the hand and wrist. Curr
Pract Orthop Surg 1964
48. Parkes Static Tenodesis
(Volar Side)—With Free
Tendon Grafts
2 free tendon grafts,
from plantaris tendon,
palmaris tendon, or toe
extensors, required for
four fingers
49. Integration of Finger Flexion
Fowler tenodesis
Wrist Tenodesis Technique
Fowler
Incorporates active wrist motion
to tension static tendon grafts
Free tendon grafts sutured to
extensor retinaculum of wrist
and passed in a dorsal to palmar
direction through the
intermetacarpal spaces, volar to
the DTML, through the lumbrical
canals, and onto the lateral bands
of dorsal extensor expansion of 4
fingers
Fowler SB: Extensor apparatus of the digits
(abstract). J Bone Joint Surg Br 1949
50. Dynamic Tendon Transfers
First reported by Sir Harold Stiles and Forrester-Brown
in 1922
By passing tendon graft slips volar to deep transverse
metacarpal ligament and into lateral band of dorsal
extensor apparatus, procedure designed to improve
synchronous motion of the finger joints and duplicate
lumbrical muscle action
Stiles HJ, Forrester-Brown MF: Treatment of Injuries of Peripheral
Spinal Nerves, London: H Frowde & Hodder & Stoughton; 1922
51. Transfer of Extrinsic Finger Flexors
Superficialis Tendon Transfer Techniques and
Modifications (Stiles; Bunnell; Littler)
FDS detached , splitted, & transferred to dorsum of
fingers to extensors tendons
Removes powerful flexor of PIP joint & converts it into
extensor
Intrinsic plus deformity
52. Bunnell (1942) : rerouted both slips of all superficialis tendons
through lumbrical canals and anchored them to both sides of
lateral band of dorsal extensor expansion (Stiles-Bunnell
procedure)
Transfer involved passage of
Split FDSI for radial side of lateral bands of index and middle
fingers
• Split FDSM for ulnar side lateral band of index, middle, and
ring fingers
• Split FDSR to radial side of ring and little fingers
• Split FDSL) to the ulnar side of little finger
Bunnell S: Surgery of the intrinsic muscles of the hand other than those producing opposition
of the thumb. J Bone Joint Surg 1942
53. Disadvantages
PIP flexion contractures and DIP extension lag in donor
finger most frequent when superficialis removed through
conventional midlateral approach
Midlateral approach exposed distal part of lateral band to
injury and contributed to DIP extension lag
High incidence of swan neck deformity in one or more of
operated fingers owing to excessive tension on transferred
tendon slip
Loss of PIP joint flexion due to adhesions between
profundus and superficialis tendon remnant
54. To prevent these complications, North and Littler : removal
of superficialis through volar incision between A1 and A2
pulleys
Brand :
Ulnar nerve palsy results in claw deformities in all four
fingers, Weakness is not limited only to fingers with
obvious clawing.
Recommendation : surgery be done in all fingers of a claw
hand
North ER, Littler JW: Transferring the flexor superficialis tendon: Technical considerations in the prevention of
proximal interphalangeal joint disability. J Hand Surg [Am] 1980
Brand PW: The reconstruction of the hand in leprosy (Hunterian lecture). Ann R Coll Surg Engl 1952
55. Modification of Bunnell
Littler proposed modification of
the Stiles-Bunnell procedure by
using FDSM
Referred to as modified Stiles-
Bunnell procedure
Tendon slips sutured under
correct tension, that is, with
wrist in neutral flexion-
extension, MP joints in 45 to 55
degrees of flexion, and IP joints
in neutral position.
Littler JW: Tendon transfers and arthrodesis in
combined median and ulnar nerve palsies. J Bone Joint
Surg Am 1949
56. 4 primary insertion sites of FDS are classified as:
A. Lateral band insertion—intrinsic replacement (Stiles
and Forrester-Brown , Bunnell , Littler , Brand , Riordan ,
Lennox-Fritschi )
B. Phalangeal insertion (Burkhalter )
C. Pulley insertion (Riordan , Zancolli , Brooks and Jones ,
Anderson )
D. Interosseous insertion (Zancolli , Palande , Anderson )
58. Phalangeal Insertion ( Burkhalter )
Insertion of superficialis tendon
slips directly to proximal
phalanx
Avoid risk of PIP joint
hyperextension noted with
transfers to lateral band of the
dorsal apparatus
Increased distance of moment
with increased flexion of MP
joint
Burkhalter WE, Strait JL:
Metacarpophalangeal flexor
replacement for intrinsic-muscle
paralysis. J Bone Joint Surg Am 1965
59. Interosseous Insertions (Zancolli Palande; Anderson)
Interosseous tendons used as insertion sites with
different motors: superficialis tendon, ECRL ,or
palmaris longus
Zancolli : first and second dorsal interosseous as
insertion sites to attach slips of a superficialis tendon
with goal of obtaining proximal phalangeal flexion
and restore digital abduction ( direct interosseous
activation)
Palande : extended this principle to correct intrinsic-
minus hands associated with reversal of the transverse
metacrapal arch
60. Pulley Insertions (Zancolli's “Lasso”)
Delineated A1 pulleys through a
transverse skin incision at level of
the distal palmar crease.
Flexor superficialis tendon
sectioned in the finger and
divided into two slips
Each tendon slip retained volar
to deep transverse metacarpal
ligament and looped through the
A1 proximal pulley and sutured to
itself
Zancolli EA: Claw-hand caused by paralysis of the
intrinsic muscles: A simple surgical procedure for
its correction. J Bone Joint Surg Am 1957;
61. Lasso procedure (ZANCOLLI) - Transfer of FDS to A-1
pulleys, index, long, ring and small fingers.
Transverse incision made at level of first A-1 pulley,
beginning at prox. palmar crease of index finger and
ending ulnarly at distal palmar crease of little finger.
67. Two slips of FDS tendon (distal) folded down volarly
over A-1 pulley and ends separately interwoven into
prox portion of FDS using tendon braider.
68. Anchored to itself with multiple horizontal
mattress stiches creating a strong lasso
69.
70.
71. Anderson : Extended
pulley insertion (EPI) by
looping slip of
superficialis tendon around
both the A1 and proximal
A2 pulleys in each finger
. Anderson GA: Analysis of paralytic claw
finger correction using flexor motors into
different insertion sites. Master's thesis,
University of Liverpool, 1988.
72. Finger Level Extensor Motor
Fowler transfer
Extensor Indicis Proprius
and Extensor Digiti
Minimi Transfer
(Fowler )
EIP and EDM tendons as transfers
lateral bands of the dorsal apparatus
May produce excessive tension in
extensor apparatus and lead to
intrinsic-plus deformities.
May cause reversal of normal
metacarpal arch and, occasionally,
extensor weakness in the little finger
Fowler SB: Extensor apparatus of the digits (abstract).
J Bone Joint Surg Br
73. Riordan Modification
Splitting EIP into 2 slips
and transferring them
through intermetacarpal
space between the ring and
little digits, routed palmar
to the transverse
metacarpal ligament and
onto radial lateral bands
of the ring and little
fingers
Riordan DC: Tendon transplantations in median-
nerve and ulnar-nerve paralysis. J Bone Joint Surg
Am 1953
74. Wrist-Level Motors for Proximal Phalanx Power and Integration of
Finger Flexion (Brand; Burkhalter; Brooks; Fowler; Riordan)
To simultaneously correct claw deformity and gain
grip strength, add additional muscle-tendon unit to
power train for flexion of proximal phalanx
Best achieved by transferring wrist motor or
brachioradialis to flex proximal phalanges
Require free grafts to provide sufficient length to reach
insertion site( plantaris, palmaris, fascia lata, or toe
extensors)
75. Dorsal Route Transfer of ECRB (Brand)
ECRL or ECRB lengthened by
plantaris tendon that was split
into four tails
Tendon slips passed through
intermetacarpal spaces, into the
lumbrical canal and palmar to
the DTML, to be attached to
radial lateral bands of the long,
ring, and little fingers and ulnar
lateral band of the index finger
Did not improve flattened
transverse metacarpal arch or
weakness of grip
Brand PW: Hand reconstruction in leprosy. British
Surgical Practice: Surgical Progress, London:
Butterworth; 1954
76. BRAND - uses ECRB/ECRL
Dorsal approach
Hockey stick PP incisions over tendon graft insertions
over radial aspect except index finger.
79. Periosteal longitudinal incision dorsal to distal edge of A-2 pulley 2.0 mm
drill hole through far cortex and 2.7 mm drill hole through near cortex
80. 2 transverse MC incisions over II & III; and
IV MC and chevron incision centered over
reticular level
84. Plantaris tendon divided into 4 slips and passed through
lumbrical canal and fixed to PP long tone.
Then tendon grafts are sutured to ECRB tendon which is
passed dorsal to extensor retinaculam.
87. Dorsiflexion of wrist relaxes the tendon
transfer and allows for full passive digital
extension
88. Wrist palmer flexion tightens the transfer
and impacts a tenodesis function, strongly
flexing the metacarpophalangeal joints
89. Wrist is held is full dorsiflexion, MCP joints in complete flexion.
Sutures removed at 14 days and a splint reapplied to hold wrist in 45°
of extension. MCP joints in full flexion and IP joints in extension.
Splinting until 6 weeks postop.
90. Modifications in the Volar Route Transfer
ECRL Volar Transfer With Proximal Phalanx Insertion
(Burkhalter and Strait). *
Brooks and Jones Volar Route Transfer to A2 Pulley
Insertion Site‡
Palmaris Four-Tail (PL4T) Transfer (Lennox-Fritschi )†
*Burkhalter WE, Strait JL: Metacarpophalangeal flexor replacement for intrinsic-muscle paralysis.
J Bone Joint Surg Am 1965
‡Brooks AL, Jones DS: A new intrinsic tendon transfer for the paralytic hand. J Bone Joint Surg Am
1975
†Fritschi EP: Nerve involvement in leprosy; the examination of the hand; the restoration of finger
function. Reconstructive Surgery in Leprosy, Bristol: John Wright & Sons; 1971
92. Omer single stage procedure
Thumb MCP joint
arthrodesis
Single transfer of FDSR
93. Postoperative Hand Therapy for Claw Correction
In first week patient supervised to attain and maintain
lumbrical-plus position and use a thermoplastic splint
between exercises
Over next 7 to 10 days active IP joint flexion begun while
MP joints remain in flexion
At no point during first and second stages patient
allowed to extend MP joints
During third stage patient encouraged to maintain IP
joint in absolute neutral extension and then extend MP
joints
Exercises at this stage combined with supervised light
functional activities that encourage lumbrical posture
94. Thumb Adduction Techniques
Adduction of thumb necessary for strong pinch
Adductor pollicis paralyzed
Brachioradialis (Boyes)
FDSR ( Brand)
FDSR (Royle –Thompson )
FDSM as Motor With Dual Insertion to the Thumb
(Goldner)
ECRB (Smith)
Combination of EI and ED (Little) Tendon Transfers for
Pinch (Robinson et al)
95. Brachioradialis as Motor (Boyes )
Tendon graft attached to
adductor tubercle of
proximal phalanx
Free end routed along volar
surface of paralyzed adductor
to third intermetacarpal
space
Graft passed deep to
extensor tendons to emerge
in a subcuticular plane on
radial side of forearm
Brachioradialis detached
through separate incision
and attached to distal graft
96. Brand transfer for Thumb adduction
Sublimis of ring finger as
motor
Traverses palm
superficial to fascia and
inserts on radia aspect at
MCP joint of thumb
97. Modified Royle-Thompson to restore thumb adduction
FDSR as motor
Split into 2 slips
1 slip to EPL distal to
MCP joint
2nd slip to adductor
pollicis
99. Restoration of Index Abduction
Thumb more important in pinch , but index finger needs
to be stabilized to provide effective pinch
For tip pinch, index finger in abduction and slight radial
rotation
Provides substitute for first dorsal interosseous muscle
Accessory Slip of APL Transfer (Neviaser et al )
EIP to first dorsal interosseous muscle (Bunnell)
Extensor Pollicis Brevis (EPB) Transfer
Palmaris Longus to the First Dorsal Interosseous
FDSR Transfer (Graham and Riordan)
100. EPB Transfer Accessory Slip of APL Transfer
Bruner (Neviaser et al )
101. Stabilization of Thumb MP and IP Joints to Restore Pinch
Split FPL to EPL Transfer-Tenodesis (Tsuge and Hashizume
; House and Walsh)
To make pulp pinch possible with thumb, necessary to
correct problem of IP joint hyperflexion & MP joint
stabilization
Split transfer of FPL neutralizes IP joint without
weakening pinch power
Tsuge K, Hashizume C: Reconstruction of opposition in the paralyzed thumb. In:
McDowell F, Enna CD, ed. Surgical rehabilitation in leprosy, Baltimore: Williams &
Wilkins; 1974:
House JH, Walsh T: Two-stage reconstruction of the tetraplegic hand. In: Strickland
JW, ed. The Hand—Master Techniques in Orthopedic Surgery, Philadelphia:
Lippincott-Raven; 1998
102. Half of FPL tendon transfer to the EPL tendon for restoring stability
to the MP joint and IP joint of thumb to improve pinch
Zigzag incision on the
volar aspect of the
thumb to expose the FPL
Radial half of FPL
sectioned distal to A2
pulley, and slit farther
proximally to the distal
end of A1 pulley
Transferred dorsally and
sutured to EPL tendon
just proximal to IP joint
103. Arthrodesis of Thumb Joints
Stabilizes key pinch and improve tip pinch
Simultaneously restore complex flexor-pronator
function of FPB and adductor-supinator function of
adductor pollicis with tendon transfers
Enable extrinsic flexor and extensors to better stabilize
remaining joint
Fixed deformity of remaining joint ia contraindication
for arthrodesis of either one
104. Arthrodesis of
MP joint
Indicated when there is severe
hyperextension contracture or
excessive Jeanne's sign with pain
and instability.
Indicated when positive Jeanne
sign develops after FDS transfer
Place MP joint in 15 degrees of
flexion, 5 degrees of abduction,
and 15 degrees of pronation
105. RESTORATION OF TRANSVERSE METACARPAL ARCH
Normal stability of distal transverse metacarpal arch lost owing
to paralysis of the interossei, and the hypothenar muscles
Metacarpals remain together as though held by transverse sling,
strong deep transverse metacarpal ligaments, while fingers are
in collapsed state
Abolishes ability of palsied hand to contour itself around object
placed within its domain
Simple act of opening lid of a jar or turning a valve becomes
clumsy and palm is unable to be “cupped” to hold fluid, gather
grain, or mold dough.
Even claw hand corrected by lumbrical replacement procedure
likely to recur if transverse metacarpal arch remains unstable or
flat
107. LITTLE FINGER ABDUCTION (Blacker et al[; Goldner ; Voche and Merle)
EDM has potential to abduct little finger through its
indirect insertion into abductor tubercle on proximal
phalanx.
Third palmar interosseous counters this effect in
normal hands
In ulnar nerve palsy intrinsic paralysis leaves the EDM
unopposed (Wartenberg's sign)
108. Split-EDM Transfer
Ulnar half of tendon is
directed volar to the deep
transverse metacarpal
ligament and sutured to the
phalangeal attachment of the
radial collateral ligament of
the MP joint of the little
finger
If little finger is clawed as
well as abducted, the other
half tendon is inserted
through the A2 pulley of the
flexor sheath.
109. High Ulnar Nerve palsy
Need to first restore
extrinsic power before
providing prehension
with intrinsic muscle
functional transfers
FDSR must not be
transferred
110. Side-to-side transfer of FDPM to FDPR and FDPL just
proximal to flexor zone V in distal forearm
Exaggerate claw deformity
After 3 weeks of immobilization, muscle strengthening
exercises supervised for next 4 weeks, knuckle bender
splint worn
Palmaris longus to FCU, in absence of palmaris longus,
section ulnar half of FCR just proximal to wrist crease
and split it proximally for 10 to 12 cm before
transferring this to FCU
111. RESTORATION OF SENSIBILITY
Loss of sensibility in ulnar border of hand and loss of
proprioception in little finger significant functional
limitations
Repeated ulceration at tips of digits can lead to
absorption and shortening
In patients who have leprosy, successful medical
treatment does not restore sensation and their
insensate digits remain liability for life
112. Digital Nerve Transfer (Lewis et al ; Stocks et al)
Lewis
Transferred functioning median-supplied digital nerve to
a nonfunctioning ulnar digital nerve of little finger to
restore sensation
Advantages in late-presenting ulnar nerve injuries and in
cases in which patients already show telltale signs of
trophic changes
Transfer of neurovascular cutaneous island flap from ulnar
side of pulp of middle finger to pulp of little finger in
selected patients with history of chronic ulnar nerve injury
due to trauma or burns
Lewis Jr RC, Tenny J, Irvine D: The restoration of sensibility by nerve translocation. Bull Hosp Jt Dis
Orthop Inst 1984
114. WASTED INTERMETACARPAL SPACES
Disfiguring and disturbing to patients, despite successful
functional restoration
Surgical insertion of dermal graft can mask interosseous
wasting and most successful between thumb and index
metacarpals
Suitable candidates : who had motor component of
deformities corrected 2 to 3 months previously with
appreciable functional restoration
116. Combined low median and ulnar palsy
Complete anesthesia of
palm and loss of
function of all intrinsics
of the fingers
If untreated, skin and
joint contractures
develop, and total claw
hand
117. Restoration of opposition of thumb
Necessary for pinch
Opposition of thumb : abdduction of thumb, flexion of
MCP joint, pronation of thumb,radial deviation of
proximal phalanx of thumb on metacarpal, motion of
thumb towards fingers
Abductor pollicis brevis
FDSR ( Riordan, Brand )
EIP ( Burkhalter)
FCU +FDSR (Groves and Goldner )
PL (Camitz )
Abductor Digiti Quinti ( Huber, Littler )
118. Riordon transfer
Sublimis tendon
of the ring finger
Pulley in FCU
Small tunnel for
insertion of the
transfer by in the
abductor pollicis
brevis tendon
119. Brand transfer to restore opposition
FDSR as motor
Tendon passed to MCP
joint & attached to
proximal and distal to
joint after splitting its
end
120.
121. Combined High Median and Ulnar Nerve Palsy
Entire hand anesthetic except for the dorsal surface
Muscles available for transfer are muscles innervated
by the radial nerve—the brachioradialis, the extensor
carpi radialis brevis, the extensor carpi radialis longus,
the extensor carpi ulnaris, and the extensor indicis
proprius
122. Omer recommended
Arthrodesis of MCP joint of thumb;
Zancolli capsulodesis of MCP joints of all fingers
Release of flexor tendon sheaths
Transfer of ECRL around radial side of wrist to FDP
Transfer of brachioradialis to FPL
Transfer of ECU, prolonged with a free graft,
around the ulnar border of the forearm to EPB
123. To restore sensibility
to the palm, Omer
suggested
amputating the
index finger and its
metacarpal and
folding the radially
innervated dorsal
flap into the palm