White spot lesions
•
163 likes•47,307 views

This presentation is intended to give the GP dentists as well as specialists some essential information regarding " white spot lesions" ,which can be considered as one of the most common side effect of orthodontic treatment with fixed appliances.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (14)
Similar to White spot lesions
Similar to White spot lesions (20)
Recently uploaded
Recently uploaded (20)
White spot lesions
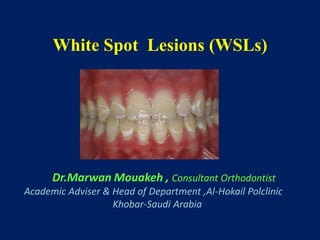
- 1. White Spot Lesions (WSLs) Dr.Marwan Mouakeh , Consultant Orthodontist Academic Adviser & Head of Department ,Al-Hokail Polclinic Khobar-Saudi Arabia
- 2. White spot lesions (WSLs) Definition : • Decalcification of the enamel surface adjacent to fixed orthodontic appliances .
- 3. White spot lesions ( WSLs ) • A Prevalent iatrogenic effect of orthodontic therapy • Incipient carious lesions develop around brackets and bands usually near the gingival margin .
- 4. Classifications of White Lesions on Enamel • Dental Fluorosis • Opacities • White Spot Lesions
- 5. • Dental Fluorosis White / yellowish lesion Not well defined Symmetrical distribution Associated with cumulative fluoride intake during enamel development . Characteristics
- 6. Dental Fluorosis Mild Fluorosis Severe Fluorosis • Affected teeth are less susceptible to dental caries .
- 7. • Enamel opacities (VS , Fluorosis) More defined shape. Well differentiated from surrounding enamel. Often located in the middle of the crown. Randomly distributed .
- 8. Enamel Hypomineralization Well demarcated opacities on the labial surface, due to injury or infection of the deciduous teeth, which has affected mineralization of the permanent teeth .
- 9. White spot lesions ( WSLs ) • Subsurface enamel porosity from carious demineralization . • Manifesting as a milky white opacity on the enamel.
- 10. Initial lesions : • white decalcification with beginning enamel breakdown • affecting the primary teeth , not associated with orthodontic treatment . Early Childhood Caries White spot lesions (WSLs) to be differentiated from
- 11. • A small lesion (score 2), severe lesion (score 3), and cavitation (score 4). No lesion is recorded as score 1. Classification of WSLs according to Gorelick and coworkers
- 12. • Overall prevalence of WSLs related to fixed appliance treatment ranges widely from 2 % - 96 % • Significant increase in prevalence with orthodontic treatment (72 % - 84 %) Prevalence of WSLs • 49.6 % in orthodontic patients ( Ogaard et al AJO-O 1989) • 24 % in an untreated controls ( Gorelick et al AJO-O 1982) •Increased with Age and Treatment duration .
- 13. Etiopathogenesis of WSLs • Areas of Demineralized Enamel developed due to prolonged plaque accumulation .
- 14. Factors Necessary for Caries Development
- 15. Formation of WSLs Fixed orthodontic appliance Rapid increase in dental plaque Low pH Increased cariogenic risk of S.mutans Acid by-products Additional lowering of pH Decalcification of enamel
- 16. Development of WSLs Plaque accumulation Low pH adjacent to orthodontic brackets Inhibition of remineralization and consequently decalcification Streptococcus mutans
- 18. Risk Factors • Inadequate oral hygiene . • Inappropriate diet (refined sugar, frequent snacks) • History of recent caries lesions or high DMFS. • Lack of adjunctive preventive measures ( fluoride or antibacterial exposure , xylitol , calcium – derived supplements ) . • Orthodontic treatment time( fixed appliances) > 36 months
- 20. External (outer) surface Internal loss of minerals The WSL’S chalky appearance is an optical phenomenon caused by mineral loss in the subsurface and the surface of the enamel
- 21. • Alteration of the enamel refractive index is the consequence of both : - surface roughness & loss of surface shine , plus - alteration of the internal reflection •Porous enamel scatters more light than sound enamel . • Visual Enamel Opacity ??
- 22. Wet Dry •Porous enamel scatters more light than sound enamel .
- 23. Fluorescence methods – QLF – Infra-red Fluorescence Transillumination Electrical Conductance – ECM Digital Radiography – DDR • Diagnostic Methods
- 24. •Fluorescence Example White Spot Reflections obscuring image
- 25. Location of WSL High prevalence on the cervical and middle thirds of the crowns : 1st Molars maxillary lateral incisors mandibular incisors and canines. Mainly on the vestibular surfaces
- 26. • The highest incidence of WSLs at the labio – gingival area of the maxillary lateral incisors . • A strong relationship between resistance to WSL formation and the rate of salivary flow . Location of WSLs
- 27. Differential Diagnosis of WSLs - Carious , vs , Non carious Lesions Procedure : Clean & dry the teeth Carefully evaluate the lesion ( magnification & lightning )
- 28. Differential Diagnosis of WSLs Carious , vs , Non carious Lesions Carious lesions : appear Rough ,Opaque ,and Porous Noncarious lesions : Smooth & Shiny appearance
- 29. Evolution of WSLs • WSL left untreated after removal of a fixed appliance will naturally reduce in size with no intervention . • About 75 % of the small lesions will regress during 6 months after debonding provided the application of caries – preventive program .
- 30. • Remineralization that could occur a few weeks following the completion of orthodontic treatment ,it is the result of improved oral hygiene and from the available minerals in saliva, fluoridated toothpaste ….
- 31. • Discoloration of white spot lesions . • Evolution of WSLs • Cavitation due to white spot lesions .
- 32. Prevention & Treatment of WSLs
- 33. Decalcification of enamel Prevention • Oral hygiene • Dentifrices • Mouth rinses • Varnishes
- 34. • Decalcification of enamel Prevention • Good Oral hygiene • Mouth rinses
- 35. White Spot Lesions… Can be Remineralized with • Changes in diet • Fluoride varnish • Daily brushing with fluoride toothpaste.
- 36. Fluoride • Inhibits demineralization • Enhances remineralization • Inhibits plaque bacteria • Prevention of WSLs
- 37. Demineralization <------------ > Remineralization •Frequent carbohydrate intake •Frequent exposure to acids •Plaque presence •Decreased salivary flow •Exposure to fluoride •Removal of plaque •Balanced diet •Limited exposure to carbohydrates
- 38. • Ways to Obtain Fluoride: Topical Fluoride Toothpaste Fluoride Varnish Fluoride Mouthrinses
- 39. Decalcification of enamel Prevention : F . Dentifrices Sodium Fluoride Amine Fluoride Monofluorophosphate Stannous Fluoride ( + Plaque inhibiting effect )
- 40. •Decalcification of enamel Prevention : F. Dentifrices • Fluoride concentration , 0.11% - 0.15% twice daily : Reduce demineralization and Enhance remineralization
- 41. • Fluoridated mouth rinses ( Na.F 0.05 %) : An improved cariostatic effect if combined with Antibacterial agents : - Chlorhexidine : inhibits plaque formation ( - ) : Tooth discoloration , metallic taste - Triclosan ( with Zinc ) : antibacterial + anti- inflammatory effects . • Prevention of WSLs
- 42. Highly concentrated topical fluoride treatment (22,600 ppm) Can reverse early white spot lesions. • Temporary discoloration of teeth and gingival tissue • Decrease enamel decalcification 44.3 % • Varnishes • Prevention of WSLs
- 43. Fluoridated Sealants , Primers and Adhesives • G.I Cements: Sustained F. Release in plaque around brackets . • Prevention of WSLs
- 44. Fluoridated Sealants , Primers and Adhesives • Resin reinforced GIC = Better bond strength • Prevention of WSLs
- 45. • Complicated designed appliances make oral hygiene difficult to carry out. • Prevention of WSLs
- 46. • Use of S.S ligatures > Elastic modules • Coil spring traction > Elastic chains … • Prevention of WSLs
- 47. • Self-ligating Brackets ….. • Prevention of WSLs
- 48. • Use of Bondable Buccal Tubes ….. • Prevention of WSLs
- 49. •Excess bonding material retains plaque. • Prevention of WSLs
- 50. • Indirect Bonding and / or Light-cure Technique….. • Prevention of WSLs
- 51. Treatment protocols for WSLs •First , Allow Natural Remineralization.
- 52. Treatment of WSLs • Avoid high concentration of F agents since they arrest enamel remineralization . • Allow Remineralization of enamel by Saliva (less visible lesions) .
- 53. Treatment of WSLs • Shows a lower right canine, which had an orthodontic white spot lesion that was treated at debond with strong fluoride varnish. The lesion has not regressed and has stained brown.
- 54. Treatment of WSLs • Low doses of F applications (50 – ppm F. mouth rinses). • Tooth Whitening “ Bleaching “ • Use of CPP –ACP “ Casein derivates “ • Enamel Microabrasion • Cosmetic Restorations ( Veneers ) .
- 55. Treatment methods • F. mouth rinses : 0.05% Na F + Chlorhexidine . • Topical F. gel or varnishes application
- 56. Topical Application of Titanium Tetrafluoride ( solution ) : the mechanism of interaction with the enamel Strong Ti-O-Ti chains on the enamel surface . A titanium-rich , glaze –like coating formed on the enamel surface following the application of Ti. Tetra F. Treatment of WSLs
- 57. • Chlorhexidine mouthwash • Antimicrobial therapy . • To achieve a shift from : Unfavorably biofilm favorably biofilm • Maybe used as a complement to F. therapy. Drawback : the tendency to stain the teeth
- 58. • Casein Phosphopeptide Amorphous Calcium Phosphate (CPP-ACP ) Treatment of WSLs
- 59. • Casein Phosphopeptide Amorphous Calcium Phosphate (CPP-ACP ) • Trade name : Recaldent • Derived from milk caseine • Enhances formation of calcium phosphate crystals
- 60. Recaldent CPP-ACP : • Natural milk derived product containing casein phosphopeptides CPP and amorphous calcium phosphates ACP
- 61. Treatment of post-orthodontic white spot lesions with casein phosphopeptide-stabilised amorphous calcium phosphate . Brochner et al, Clin Oral Invest, April 2010 The mean area of the WS lesions decreased by 58% in the CPP- ACP group and 26% in the fluoride group .
- 62. • Casein Phosphopeptide Amorphous Calcium Phosphate (CPP-ACP ) 7 days 4 weeks 12 weeks
- 63. Recaldent CPP-ACP Chewing Gum : This gum contains the active CPP-ACP . Recaldent also contains Xylitol, which is a natural sweetener shown to help control mouth bacteria and improve saliva quality. •The in vivo studies of the remineralization properties of Recaldent (CPP-ACP) Gum have shown subsurface mineral gain can occur by chewing the gum for periods of 15 minutes for 2 weeks.
- 64. • Vital Tooth Bleaching Treatment of WSLs
- 65. •Vital Tooth Bleaching •View of the same maxillary anterior teeth following 4 weeks of overnight vital bleaching with 10% carbamide peroxide delivered in a custom tray. Treatment of WSLs
- 66. • View of the same maxillary anterior teeth following 4 weeks of bleaching , 30 minutes twice per day, with a hydrogen peroxide gel impregnated on polyethylene strips. •Vital Tooth Bleaching
- 67. Microabrasion of the enamel Treatment of WSLs
- 68. Microabrasion • A technique to remove the superficial non- carious superficial enamel defects as well as WSL . • Topical application of an 18 % hydrochloric acid and pumice , 1 – 2 minutes .
- 69. Microabrasion • 5 to 10 applications of the microabrasion compound should be effective . • The abraded enamel surface is less susceptible to demineralization than natural enamel . • Following the microabrasion technique , a 4-minute 2 % Na F treatment is recommended .
- 70. • Cosmetic Restorations in Severe Cases Treatment of WSLs
- 71. Decalcification restored with composite resin . • Cosmetic Restorations ( ICon ): Caries Infiltration with light-curable resin for non-cavitated lesions
- 72. • Patient who needed composite buildups on the maxillary anterior teeth to esthetically improve areas of severe decalcification following orthodontic treatment . • Cosmetic Restorations
- 74. How Do You Proceed ? Problem : Inadequate oral hygiene, generalized gingivitis, plaque accumulation, and white spot lesions at the bucco-cervical surfaces.
- 75. Discuss with the patient the risk factors, Make recommendations according to the problems (eg, diet and oral hygiene behavioral assessment), Prescribe high-fluoride (5000 ppm) toothpaste and 0.12% chlorhexidine rinses, and Reevaluate in few months to assess whether patient has been compliant and able to proceed with orthodontic treatment . How Do You Proceed ?
- 76. What do you recommend? Reevaluate the risk factors Reinforce oral hygiene instructions, Prescribe high-fluoride toothpaste and chlorhexidine rinses, Apply fluoride varnish at least 2 or 3 times a year, and also Recommend frequent use of xylitol or sugar-free gum.
- 77. Problem : at the debonding appointment , you note white spot lesions and areas of cavitation on the patient. What do you do?
- 78. Summary : Treatment protocols for WSLs • First , allow natural remineralization. • Low doses of F applications (50 – ppm F. mouth rinses). •Use of CPP –ACP “ Casein derivates “ • If the lesions persist , professional bleaching is indicated. • If the effect of bleaching is inadequate , Microabrasion is an option. • Lastly , direct or indirect Veneers could be considered.
- 79. Conclusions : • To prevent development of white spot lesions, orthodontists should assess each patient’s risk factors before and during treatment. • Oral hygiene instructions are important, but patients might need to be assisted with additional measures, including fluoride varnish, chlorhexidine , dietary modification, or calcium-containing remineralization products that can help prevent enamel demineralization, enhance remineralization, and modify patient and biofilm factors.
- 80. Conclusions : • Restorative treatment for established white spot lesions can range from the most conservative (remineralization with fluoride, calcium, and phosphate) to the most aggressive (tooth reduction and porcelain veneers).
- 81. Conclusions : It is crucial to establish a caries risk assessment and recommendation protocol for patients before, during, and after treatment to be able to provide overall successful orthodontic treatments for them.
- 82. Thank You … Dr.Marwan Mouakeh Syria –Aleppo, the public park