Evaluating Orphan and Vulnerable Children Outcomes: Innovative Methodology for, and Results of, Pilot Testing a New Toolkit
•
1 like•587 views

Presented at the International AIDS Conference in July 2014.
Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Evaluating Orphan and Vulnerable Children Outcomes: Innovative Methodology for, and Results of, Pilot Testing a New Toolkit
Similar to Evaluating Orphan and Vulnerable Children Outcomes: Innovative Methodology for, and Results of, Pilot Testing a New Toolkit (20)
More from MEASURE Evaluation
More from MEASURE Evaluation (20)
Recently uploaded
Recently uploaded (20)
Evaluating Orphan and Vulnerable Children Outcomes: Innovative Methodology for, and Results of, Pilot Testing a New Toolkit
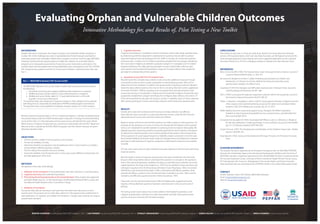
- 1. Evaluating Orphan and Vulnerable Children Outcomes Innovative Methodology for, and Results of, Pilot Testing a New Toolkit JENIFER CHAPMAN Futures Group/MEASURE Evaluation, USA // LISA PARKER Futures Group/MEASURE Evaluation, USA // STANLEY AMADIEGWU Futures Group/MEASURE Evaluation, Nigeria // SHEHU SALIHU Futures Group/MEASURE Evaluation, Nigeria // MWILA KANEMA Futures Group, Zambia BACKGROUND Despite high donor investment, the impact of orphan and vulnerable children programs is unclear. Part of the challenge was a lack of standardized and tested measures and tools for evaluating orphan and vulnerable children (OVC) program outcomes. To fill this gap, MEASURE Evaluation produced three questionnaires to enable the collection of actionable data for programs and comparative assessments of outcomes across interventions and regions. The questionnaires were developed with strong stakeholder input, and aligned to the 2012 PEPFAR OVC Programming Guidance and the U.S. Government Children in Adversity Action Plan (see Box 1). Box 1—MEASURE Evaluation OVC Survey Toolkit The MEASURE Evaluation OVC survey toolkit includes three questionnaires that measure the following: 1. Household outcomes and caregiver wellbeing (administered to a caregiver). 2. Wellbeing among children aged 0–9 years (administered to a caregiver). 3. Wellbeing among children aged 10–17 years (administered to a child with guardian consent and child assent). The questionnaires were designed to measure changes in child, caregiver and household well-being that can reasonably be attributed to PEPFAR-funded program interventions. The questionnaires may be applied in evaluation, situation analysis, or in other research. We pilot tested the questionnaires in 2013 in Zambia and Nigeria. In Zambia, we piloted tested the questionnaires under the USAID-funded impact evaluation of savings and internal lending communities (SILC) on child well-being, led by Futures Group with World Vision and Catholic Relief Services. In Nigeria, the pilot test was conducted in partnership with the PACT Rapid and Effective Action Combatting HIV/AIDS (REACH) program and the Catholic Dioceses of Lafia in Akwanga, Nasawara State. OBJECTIVES • Test the construct validity of some questions and concepts. • Pre-test the reliability of scales. • Determine whether any questions may be duplicative and, in some instances, to enable a choice between different question versions. • Test the clarity of the question sets as an entirety. • Assess the reliability of recall periods and, in some cases, assess different recall periods; and test field application of the tools. METHODS We applied a three-step methodology: 1. Validation of the translation of the questionnaire with data collectors in a training setting. 2. Cognitive interviews with potential respondents. 3. Pilot-testing the full questionnaires at the household level. These studies were approved by Health Media Labs, Inc., in the United States, the Biomedical Research IRB in Lusaka, and the National Health Research Ethics Committee in Abuja. 1. Validation of Translation During the data collector training for each pilot test, the trainer led a discussion on each questionnaire. The purpose was to orient data collectors to the questionnaire, enable them to seek clarification on measures, and validate the translation. Changes were made by the original questionnaire translator. 2. Cognitive Interview Cognitive interviewing is a qualitative research technique used to help design questionnaires by determining whether respondents understand the questions and are able to produce expected responses (de Leeuw, Borgers & Smits, 2004). In Zambia, we conducted cognitive interviews with 12 adults and 16 children purposively sampled from the program beneficiary list in one ward. In Nigeria, we selected a purposive sample of 12 caregivers and 16 children program beneficiary lists. After gaining participant consent, trained data collectors read each question and recorded the participant’s response. The data collector then probed for participant’s understanding of the question. 3. Household Survey Pilot Test of Complete Tools We pilot tested the complete data collection tools and a few additional measures through a household survey pre-test to assess respondent’s understanding, question flow, and to determine the time needed to complete a full questionnaire, including recruitment. We pilot tested the data collection process from start to finish, including informed consent, application of the Kish Grid (Kish, 1949) for sampling at the household level, and administration of all survey tools among 21 households in Zambia and 20 households in Nigeria. Households were purposively sampled from program beneficiary lists. In Nigeria, data collectors returned to 10 of the 20 households the day after the survey to conduct a reliability check of 16 key measures. After gaining participant consent, trained data collectors administered the questionnaires. RESULTS Overall, items were well understood and the process of data collection was efficient. Data collectors were successful in conducting informed consent, using the Kish Grid, and administering the survey tools with both adults and children. Based on results and lessons learned from piloting, we made changes to a few questions. For example, for the questions on access to money we changed the formulation of the question to focus on a respondent’s specific experience accessing money to improve data quality. We adapted questions requesting whether household expenditures had increased or decreased by splitting the original questions and including additional skip patterns. We changed three of four questions on social support based on a reliability analysis conducted on the full scale from the Rand Medical Outcomes study. Finally we changed various recall periods to improve participant understanding and response categories to add frequent responses not originally included. Of note, Likert scales were not well understand and were replaced in the final tools with binary response options. We pilot tested a variety of measures and questions that were omitted from the final tools because either respondents did not understand the questions or concepts in the questions well or they demonstrated poor variability, including: an extended asset schedule, two social capital questions, the Hope Scale (Snyder et al, 1997) and two additional hope questions, two self-esteem questions from the Rosenburg Self-Esteem Scale (Rosenburg, 1965), the General Self-Efficacy scale (Schwrzer & Jerusalem, 1995), a stand-alone self-efficacy question, three parental self-efficacy questions from the Parental Stress Scale (Berry & Jones, 1995), and the strengths and difficulties questionnaire for children (Goodman, 1997). There were very few questionnaire revisions after the Nigeria pilot, suggesting that the majority of the problematic questions had been corrected prior to this second round of piloting. Pre-testing raised concern about how to best address child-headed households, as the caregiver questionnaire is tailored to an adult respondent, and both child questionnaires assume a previous interview with the adult caregiver. CONCLUSIONS Pilot testing of new tools is critical, yet rarely done. Results from these pilot tests informed revision of the questionnaires, which are now ready for public use. We highly recommend this three-pronged approach to pilot testing, with some suggested adaptations to the Cognitive Interviews (Parker et al., 2014), to colleagues seeking to validate their data collection tools. REFERENCES Berry JO, & Jones WH (1995). The Parental Stress Scale: Initial psychometric evidence. Journal of Social and Personal Relationships, 12, 463–472. de Leeuw ED, Borgers N, & Smits A. (2004). Pretesting questionnaires for children and adolescents. In S Presser, et al., (Eds.), Methods for testing and evaluating survey questionnaires. Hoboken, NJ: Wiley & Sons. Goodman R (1997) The Strengths and Difficulties Questionnaire: A Research Note. Journal of Child Psychology and Psychiatry, 38, 581–586. Kish L (1949). A procedure for objective respondent selection within the household. Journal of the American Statistical Association 44(247): 380–87. Parker L, Chapman J, Amadiegw S, Salihu S (2014). Using cognitive interviews in Nigeria to pre-test child, caregiver, and household well-being survey tools for orphan and vulnerable children programs. AIDS 2014, Melbourne, Australia, July 20–25, 2012. RAND. Medical Outcomes Study Social Support Survey. Arlington, VA: RAND Corporation. Available at: http://www.rand.org/health/surveys_tools/mos/mos_mentalhealth.html (last accessed April 2013). Schwarzer R, & Jerusalem M (1995). Generalized Self-Efficacy scale. In J. Weinman, S. Wright, & M. Johnston, Measures in health psychology: A user’s portfolio. Causal and control beliefs (pp. 35–37). Windsor, England: NFER-NELSON. Snyder CR, et al., (1997). The Development and Validation of the Children’s Hope Scale. J Pediatr Psychol. 22(3):399–421. Rosenberg M. (1965). Society and the Adolescent Self-image. Princeton, NJ: Princeton University Press. ACKNOWLEDGEMENTS This research has been supported by the President’s Emergency Plan for AIDS Relief (PEPFAR) through the United States Agency for International Development (USAID) under the terms of MEASURE Evaluation cooperative agreement GHA-A-00-08-00003-00 which is implemented by the Carolina Population Center, University of North Carolina at Chapel Hill with Futures Group, ICF International, John Snow, Inc., Management Sciences for Health, and Tulane University. Views expressed are not necessarily those of PEPFAR, USAID, or the United States government. CONTACT Jenifer Chapman, Senior OVC Advisor, MEASURE Evaluation Email: jchapman@futuresgroup.com Website: measureevaluation.org Evaluation