1. Adrenal Revision
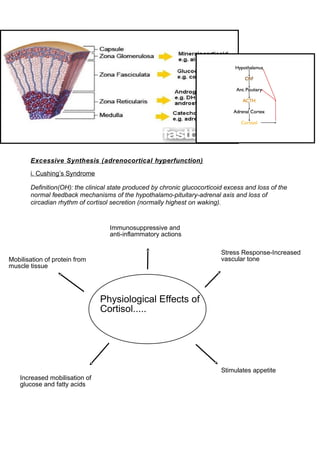
Excessive Synthesis (adrenocortical hyperfunction)
i. Cushing’s Syndrome
Definition(OH): the clinical state produced by chronic glucocorticoid excess and loss of the
normal feedback mechanisms of the hypothalamo-pituitary-adrenal axis and loss of
circadian rhythm of cortisol secretion (normally highest on waking).
Physiological Effects of
Cortisol.....
Stress Response-Increased
vascular tone
Stimulates appetite
Increased mobilisation of
glucose and fatty acids
Immunosuppressive and
anti-inflammatory actions
Mobilisation of protein from
muscle tissue
2. Think about the physiological effects of cortisol and what symptoms/signs this might
produce:
Signs
Central obesity
Plethoric (red) moon face
Buffalo neck hump
Supraclavicular fat pads
Skin and muscle atrophy
Bruises
Purple abdominal striae
Osteoporosis
Hypertension
Hyperglycaemia
Infection prone-poor healing.
Symptoms
Increase in weight
Mood change (depression, lethargy, irritability)
Weakness
Irregular periods
Facial hair growth (in females)
Erectile dysfunction
recurrent Achilles tendon rupture
3. What are the causes?
• Iatrogenic
The commonest cause is oral steroid treatment (i.e. after long-term treatment with
prednisolone and dexamethasone)
• Endogenous
The endogenous causes can be divided into:
-Adrenal origin (excess cortisol production by an adrenal cortical neoplasm, e.g. adrenal
nodular hyperplasia)
-Pituitary origin (excess ACTH production by a pituitary neoplasm-Cushing’s disease)
-Ectopic origin (excess ACTH production by a non-pituitary neoplasm, especially small cell
lung cancer and carcinoid tumours).
How do you tell which is which?
• dexamethasone suppression test: in Cushing’s syndrome the cortisol does not fall as we
would expect it to.
• to work out where the lesion is-do a plasma ACTH; if it is undetectable, then the excess
cortisol must be coming from the Adrenals (as the pituitary is still responding to negative
feedback, resulting in the low/undetectable levels of ACTH, but the adrenals are out of
control)
• if ACTH is detectable, to distinguish between a pituitary and an ectopic cause, we need
to do a high-dose dexamethasone suppression test; complete or partial suppression of
the cortisol levels indicates a pituitary cause as the pituitary retains some feedback
control.
Treatment?
• Iatrogenic: Stop oral steroids if possible
4. • Endogenous: Selective removal of the offending neoplasm if possible; bilateral
adrenalectomy if source unlocatable, recurrence post-op, or adrenal adenoma/carcinoma
present.
ii. Conn’s Syndrome
• Primary hyperaldosteronism (Conn Syndrome) is usually caused by an aldosterone-
secreting adrenal adenoma.
*Key thing to remember regarding Conn Syndrome: it causes hypertension,
neuromuscular symptoms and renal potassium wasting due to elevated levels of
aldosterone (if you think about what aldosterone does, it makes sense).
iii. Adrenogenital Syndromes
• Congenital adrenal hyperplasia-95% of cases are due to partial or complete deficiency in
21-hydroxylase.
• The deficiency in this enzyme involved in the biosynthesis of adrenal steroids (i.e.
cortisol) means that steroidogenesis is then channelled into other pathways, leading to
excess production of androgens.
*The 3 most common syndromes are characterised by virilism-the newborn female infant
may present with pseudohermaphrodism, while precocious puberty occurs in affected
males.
*Some defects also affect aldosterone synthesis (i.e. low aldosterone as well as low
cortisol), causing salt wasting which can be life-threatening in the newborn.
Adrenal insufficiency
i.Addison’s Disease
Definition (OH): primary adrenocortical insufficiency; destruction of the adrenal cortex
leads to glucocorticoid (cortisol) and mineralocorticoid (aldosterone) deficiency.
What are the causes?
Surgical Sieve is helpful here:
5. • V vascular-perinatal haemorrhagic necrosis, adrenal haemorrhage (Waterhouse-
Friderichsen syndrome), post partum adrenal infarction
• I infection/inflammatory-chronic infections (T.B. is commonest cause worldwide),
sarcoidosis
• T trauma-traumatic necrosis
• A auto-immune-auto-immune adrenalitis (60-70%, now commonest cause in U.K.)
• M metabolic-amyloidosis (not really a metabolic condition but may help to remember it
here, or you can just remember it on it’s own)
• I iatrogenic-abrupt withdrawal of corticosteroid treatment
• N neoplastic-disseminated metastatic carcinoma (lung, breast)
Presentation
• If it helps you can remember this slide and the 5 T’s:
Or this list:
• weakness
• nausea & vomiting
• abdominal pain
• weight loss
• hyperpigmentation of the skin (check palmar creases) & mucous membranes
• hypotension-dizziness and faints.
• Vitiligo
Remember these electrolyte disturbances:
Hb 12.5 g/dL normal
6. Na+ 125 mmol/L (low)
K+ 6.5mmol/L (high)
Ur 10mmol/L (high)
Glucose 2.9 mmol/L (low)
Investigations:
• Short Synacthen Test-an injection of synacthen should cause a normal rise of cortisol in
30 minutes (cortisol measurement after 30 minutes should be >550nmol/L)
Treatment:
• Corticosteroid Replacement (hydrocortisone daily)
• Mineralocorticoid replacement may be needed as well (fludrocortisone daily)
• Warn against abruptly stopping steroids, and advise about need to increase doses in
illness/stress
• Give steroid card
Management of an Addisonian Crisis:
D-assess for danger
R-assess for a response (pt may be very weak and confused)
A-Airways-look, listen, feel.
B-Breathing-look, listen, feel, measure (O2 sats), treat (oxygen)
C-Circulation-look (pallor, oedema, bleeding), listen (heart sounds-may be soft), measure
(BP-they are likely to be hypotensive, HR-feeble rapid pulse, UO-may be oliguric, Temp-
7. pyrexia is common and may be due to underlying infection, Cap refill), treat (obtain iv
access, give bolus of normal saline, take bloods)
D-Disability-AVPU score, measure serum glucose
E-Exposure-hyperpigmentation/medic alert bracelet may give you some clues!
• If an Addisonian crisis is suspected, treat without waiting for biochemical results
• Take blood for cortisol and ACTH if possible
• Give Hydrocortisone sodium succinate 100mg stat.
• Glucose iv may be needed if hypoglycaemic
• Continue iv fluids to correct dehydration, as guided by clinical state. Correct electrolyte
imbalances.
• Continue hydrocortisone sodium succinate e.g. 100mg/6h iv.
• Change to oral steroids after 72 hrs if patient’s condition is good.
• Fludrocortisone may be needed as well.
• Search for and treat the underlying cause (Infection, trauma. abrupt withdrawal of
steroids)
Key Points
• In Cushing’s syndrome you have an excess of Cortisol
• To investigate this you do the dexamethasone suppression test (because you are
trying to see if the excess levels can be suppressed)
• In Addison’s disease you have Adrenal insufficiency
• This results in characteristic features including hyperpigmentation, nausea & vomiting,
weakness and hypotension.
• You get low sodium and low glucose
• You get high potassium and raised urea
• To investigate this you do the short synacthen test (because you are trying to see if
synthetic ACTH will stimulate cortisol release)