1. http://www.youtube.com/watch?v=krXoyP5j5lk - St. George’s thyroid exam
Thyroid
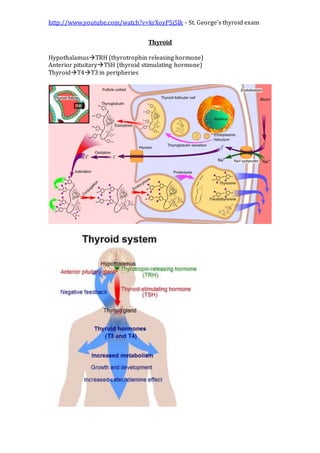
HypothalamusTRH (thyrotrophin releasing hormone)
Anterior pituitaryTSH (thyroid stimulating hormone)
ThyroidT4T3 in peripheries
2. http://www.youtube.com/watch?v=krXoyP5j5lk - St. George’s thyroid exam
Primary disease= in the thyroid itself
Secondary=in pituiaty (very rare)
Tests
Free T4 and t3 (sometimes in hyperthyroidism), more useful than total
levels as this is affected by protein carrier levels (which is affected by
drugs, pregnancy, hepatitis, nephrotic syndrome..etc)
TSH
Thyroid autoantibodies – antithyroid peroxidase and antithyroglobulin
antibodies. Maybe increased in autoimmune disease (Hashimotos or
Graves)
TSH receptor antibodies (Graves)
US – determines cystic (usually benign) from solid nodules
Isotope scan – can detect ectopic thyroid tissue or carcinoma. Hot
(increased uptake), cold and neutral nodules – hot and neutral nodules
are usually not malignant.
TSH, T4 Hypothyroidism
TSH, normal T4 Treated/subclinical hypothyroidism
TSH, T4 TSH tumour or hormone resistance
TSH, T4 Hyperthyroidism
TSH, normal T4 Subclinical hyperthyroidism
TSH, T4 Sick euthyroidism
Sick euthyroidism = deranged TFTs in illness (usually everything becomes low)
Goitre
Can be associated with hypothyroidism or hyperthyroidism. Most causes
can lead to a goitre
Most common cause worldwide is iodine deficiency
Can be caused by a diffuse enlargement (iodine) or due to nodular
enlargement (neoplasm)
Nodules can be inactive or active (aka toxic)
Hyperthyroidism
Thyrotoxicosis often used synonymously
Causes
o Autoimmune = Graves disease
o Infective = De Quervain’s thyroiditis
A self limiting, acute, severe post viral hyperthyroidism
(coxsackie, adenovirus or URTI). Leads to a
characteristically painful goitre
o Neoplastic = toxic adenoma
o Iatrogenic = drugs such as amiodarone or lithium. Also from over
treating hypothyroidism
Symptoms
o Increased metabolismweight loss and increased appetite
o Heat intolerance
o Sweating
3. http://www.youtube.com/watch?v=krXoyP5j5lk - St. George’s thyroid exam
o Diarrhoea
o Tremor
o Irritability/restlessness
o Psychosis
o Itch
o Oligomenorrhoea
Signs
o Increased pulse rate
o atrial fibrillation
o palmar erythema
o hair thinning
o lid retraction
o goiter, nodules or bruites
o Graves
eye signs – exophthalmos (abnormal connective tissue
deposition in the orbit and extraocular muscles due to
fibrosis following lymphocyte infiltration),
ophthalmoplegia (paralysis of muscles by similar
mechanism), lid retraction and lid lag. Eyelid retraction is
the most common sign of ophthalmopathy. Von Graefe's
sign (lid lag sign) is the immobility or lagging of the upper
eyelid on downward rotation of the eye. Abnormal
wideness of the eye due to retraction of both lids is called
Dalrymple’s sign and is noticed due to large area of
whiteness above and below the iris (particularly above). In
moderate active disease, the signs and symptoms are
persistent and increasing and include myopathy. The
inflammation and edema of the extraocular muscles lead to
gaze abnormalities. The inferior rectus muscle is the most
commonly affected muscle and patient may experience
vertical diplopia on upgaze and limitation of elevation of
the eyes due to fibrosis of the muscle. Protosis is a
description of bulging eyes
Pretibial myxoedema - It usually presents itself as a waxy,
discolored induration of the skin—classically described as
having a so-called peau d'orange (orange peel) appearance
thyroid acropatchy - painful clubbing of fingers or toes and
periosteal limb bone reaction
Treatments
o Medical
beta blockers for symptoms
either titrate with carbimazole
or block with carbimazole and replace with thyroxine
SE of carbimazole is agranulocytosis (can septic
neutropaenia, watch out for illness)
Propylthiouracil is another alternative
Antithyroid medicines inhibit thyroid peroxidase
Radioiodine can be used to ablate the thyroid but almost
invariably leads to hypothyroidism. Can thyroid storm
4. http://www.youtube.com/watch?v=krXoyP5j5lk - St. George’s thyroid exam
2 major contraindications to radioiodine are pregnancy and
lactation
o Surgery
Subtotal thyroidectomy
Thyroid storm - also referred to as thyrotoxic crisis, is an acute, life-
threatening, hypermetabolic state induced by excessive release of thyroid
hormones (THs) in individuals with thyrotoxicosis. Thyroid storm may be
the initial presentation of thyrotoxicosis in undiagnosed children,
particularly in neonates. The clinical presentation includes fever,
tachycardia, hypertension, and neurological and GI abnormalities.
Hypertension may be followed by congestive heart failure that is
associated with hypotension and shock. Because thyroid storm is almost
invariably fatal if left untreated, rapid diagnosis and aggressive treatment
are critical.
Graves disease
o Autoimmune – antibodies stimulating TSH receptors
o 60% have eye signs
o strong genetic component – many genes involved (incl. HLA-DR3)
o TSH antibodies not routinely tested
o Other antibodies against thyroid peroxidase and thyroglobulin in
75% of patients which can be measured using
agglutination/ELISA/immunofluorescence
Hypothyroidism
Causes
o Autoimmune
Hashimoto’s thyroiditis – goiter. Destruction of thyroid
tissue, mechanism not understood. May start as
hyperthyroidism. HLA DR4 and 3. Acute phase may be
hyperthyroidism.
Primary myxedema – no goiter, atrophy. Blocking of TSH
receptor with autoantibodies (same as Grave’s but opposite
effect). HLA DR4
o Environmental/dietary – iodine deficiency. In countries without
iodinised salt
o Iatrogenic – thyroidectomy or drugs (amiodorone, lithium)
o Congenital cretinism. Now screened for using the Guthrie heel
prick test 5 days postnatally.
Symptoms
o Tiredness
o Lethargy
o Depression
o Cold intolerance
o Weight gain
o Constipation
o Menorrhagia
o Hoarse voice
o Dementia
Signs
o Bradycardia
o Dry skin and hair
5. http://www.youtube.com/watch?v=krXoyP5j5lk - St. George’s thyroid exam
o Ataxia
o Slow reflexes
o Peripheral neuropathy
Treatment
o Replace what is missing – give levothyroxine
Thyroid function screening
o Those with other autoimmune conditions – vitiligo, Addison’s or
type 1 (or gestational) diabetes
o Those on amiodorone or lithium (6 monthly)
o Hyperlipidaemia
o Atrial fibrillation
o Certain genetic conditions that have a strong association eg
Turner’s and Down’s syndrome
Reference ranges:
Calcium 2.1-2.6 mmol/l
Phosphate 0.8-1.4 mmol/l
CRP < 10 mg/l
Thyroid stimulating hormone
(TSH)
0.5-5.5 mu/l
Free thyroxine (T4) 9-22 pmol/l
Total thyroxine (T4) 70-140 nmol/l
Amylase 70-300 u/l
Uric acid
0.18-0.48
mmol/l
SBAs
1. A 23-year-old woman presents with sweating and tremor. Her thyroid
function tests are as follows:
TSH <0.05 mU/l
Free
T4
25 pmol/l
What is the most common cause of this presentation?
A
.
Hashimoto's thyroiditis
B
.
Graves' disease
C
.
Toxic nodular goitre
D
.
De Quervain's thyroiditis
6. http://www.youtube.com/watch?v=krXoyP5j5lk - St. George’s thyroid exam
E
.
Toxic adenoma
2. A 33-year-old female is referred by her GP with thyrotoxicosis. Following a
discussion of management options she elects to have radioiodine therapy. Which
one of the following is the most likely adverse effect?
A
.
Hypothyroidism
B
.
Thyroid malignancy
C
.
Agranulocytosis
D
.
Oesophagitis
E
.
Precipitation of thyroid eye disease
3. A 36-year-old woman presents with feeling tired and cold all the time. On
examination a firm, non-tender goitre is noted. Blood tests reveal the following:
TSH 34.2
mU/l
Free
T4
5.4
pmol/l
What is the most likely diagnosis?
A
.
Primary atrophic hypothyroidism
B
.
Pituitary failure
C
.
De Quervain's thyroiditis
D
.
Iodine deficiency
E
.
Hashimoto's thyroiditis
4. A 43-year-old woman presents for follow-up in clinic. She was diagnosed with
Hashimoto's thyroiditis four months ago and is currently being treated with
levothyroxine 75 mcg od. What is the single most important blood test to assess
her response to treatment?
A
.
ESR
B
.
TSH
7. http://www.youtube.com/watch?v=krXoyP5j5lk - St. George’s thyroid exam
C
.
Free T4
D
.
Total T4
E
.
Free T3
5. A 40-year-old woman complains of feeling tired all the time and putting on
weight. On examination a diffuse, non-tender goitre is noted. Blood tests are
ordered:
TSH 15.1
mU/l
Free T4 7.1
pmol/l
ESR 14
mm/hr
Anti-TSH receptor stimulating antibodies Negative
Anti-thyroid peroxidase antibodies Positive
What is the most likely diagnosis?
A
.
Pituitary failure
B
.
Primary atrophic hypothyroidism
C
.
De Quervain's thyroiditis
D
.
Hashimoto's thyroiditis
E
.
Grave's disease
6. A 52-year-old woman who was diagnosed as having primary atrophic
hypothyroidism 12 months ago is reviewed following recent thyroid function
tests (TFTs):
TSH 12.5
mU/l
Free
T4
14
pmol/l
She is currently taking 75mcg of levothyroxine once a day. How should these
results be interpreted?
A
.
Poor compliance with medication
B Taking extra thyroxine
8. http://www.youtube.com/watch?v=krXoyP5j5lk - St. George’s thyroid exam
.
C
.
Evidence of recent systemic steroid therapy
D
.
Keep on same dose
E
.
T4 to T3 conversion disorder
Answers
1. Graves' disease is the most common cause of thyrotoxicosis in the UK. All the
other conditions can cause thyrotoxicosis but are less common.
Thyrotoxicosis
Graves' disease accounts for around 50-60% of cases of thyrotoxicosis.
Causes
• Graves' disease
• toxic nodular goitre
• subacute (de Quervain's) thyroiditis
• post-partum thyroiditis
• acute phase of Hashimoto's thyroiditis (later results in hypothyroidism)
• toxic adenoma (Plummer's disease)
• amiodarone therapy
Investigation
• TSH down, T4 and T3 up
• thyroid autoantibodies
• other investigations are not routinely done but includes isotope scanning
2. It is well documented that radioiodine therapy can precipitate thyroid eye
disease but a majority of patients eventually require thyroxine replacement
Graves' disease: management
Despite many trials there is no clear guidance on the optimal management of
Graves' disease. Treatment options include titration of anti-thyroid drugs (ATDs,
for example carbimazole), block-and-replace regimes, radioiodine treatment and
surgery. Propranolol is often given initially to block adrenergic effects
ATD titration
• carbimazole is started at 40mg and reduced gradually to maintain
euthyroidism
• typically continued for 12-18 months
• patients following an ATD titration regime have been shown to suffer fewer
side-effects than those on a block-and-replace regime
Block-and-replace
9. http://www.youtube.com/watch?v=krXoyP5j5lk - St. George’s thyroid exam
• carbimazole is started at 40mg
• thyroxine is added when the patient is euthyroid
• treatment typically lasts for 6-9 months
The major complication of carbimazole therapy is agranulocytosis
Radioiodine treatment
• contraindications include pregnancy (should be avoided for 4-6 months
following treatment) and age < 16 years. Thyroid eye disease is a relative
contraindication, as it may worsen the condition
• the proportion of patients who become hypothyroid depends on the dose
given, but as a rule the majority of patient will require thyroxine
supplementation after 5 years
3.
Hashimoto's thyroiditis = hypothyroidism + goitre + anti-TPO
The combination of a goitre with hypothyroidism points to a diagnosis of
Hashimoto's. De Quervain's thyroiditis typically causes a painful goitre.
Hashimoto's thyroiditis
Hashimoto's thyroiditis is an autoimmune disorder of the thyroid gland. It is
typically associated with hypothyroidism although there may be a transient
thyrotoxicosis in the acute phase. It is 10 times more common in women
Features
• features of hypothyroidism
• goitre: firm, non-tender
anti-thyroid peroxidase and also anti-Tg antibodies
4. Hypothyroidism: management
Key points
• initial starting dose of levothyroxine should be lower in elderly patients and
those with ischaemic heart disease (e.g. 25-50 mcg/day)
• following a change in thyroxine dose thyroid function tests should be checked
after 6-8 weeks
• the therapeutic goal is 'normalisation' of the thyroid stimulating hormone
(TSH) level. As the majority unaffected people have a TSH value 0.5-2.5
mU/l it is now thought preferable to aim for a TSH in this range
• there is no evidence to support combination therapy with levothyroxine and
liothyronine
Side-effects of thyroxine therapy
• hyperthyroidism: due to over treatment
• reduced bone mineral density
• worsening of angina
• atrial fibrillation
10. http://www.youtube.com/watch?v=krXoyP5j5lk - St. George’s thyroid exam
5. this patient has Hashimoto's thyroiditis, as evidenced by the
hypothyroidism, goitre and anti-thyroid peroxidase antibodies. De Quervain's
thyroiditis typically causes a painful goitre and a raised ESR. Around 90% of
patients with Grave's disease have anti-TSH receptor stimulating antibodies.
6. Thyroid function tests
The interpretation of thyroid function tests is usually straightforward:
TS
H
Free
T4
Thyrotoxicosis (e.g. Graves' disease) Low High In T3 thyrotoxicosis the free T4
will be normal
Primary hypothyroidism (primary
atrophic hypothyroidism)
Hig
h
Low
Secondary hypothyroidism Low Low Replacement steroid therapy is
required prior to thyroxine
Sick euthyroid syndrome* Low
**
Low Common in hospital inpatients
Poor compliance with thyroxine Hig
h
Norm
al /
high
Steroid therapy Low Norm
al
*now referred to as non-thyroidal illness
**TSH may be normal in some cases
11. http://www.youtube.com/watch?v=krXoyP5j5lk - St. George’s thyroid exam
OSCE
1. Wash hands, introduce, gain permission, expose (down to clavicles),
reposition (sitting). Ask if they have any pain
2. General inspection
a. Body habitus – overweight = hypo, under=hyper
b. Clothing – appropriate for weather? Over dressed = hypo,
under =hyper
c. Hair – greasy=hyper, dry=hypo
d. Eye brows – lost outer 2/3rds = hypo
e. Anxious/restless
3. Inspection of hands (VET SOAP)
V – vitiligo (indicator of autoimmune disease)
E – erythema of palms
T – tremor (ask patient to hold hands out and can put a piece of paper
on top to highlight fine tremor)
S - sweating
O - onycholysis
A – acropatchy – Graves disease specific
P – pulse (bradycardia=hypo, tachycardia/AF=hyper)
4. Inspection of neck
a. Scars, Sinuses, Swellings, Skin changes
b. Ask patient to stick tongue out – thyroglossal cysts move up
c. Ask patient to swallow water – goitres move up as attached to
pre-tracheal fascia
5. Inspection of eyes (Grave’s disease)
a. Look – from above and to sides do the eyes protrude beyond
the supraorbital ridge i.e. proptosis/exophthalmos
b. Ask patient to follow an H and ask them to tell you if they see
any diplopia to test for Ophthalmoplegia
c. Ask patient to follow finger from top to bottom for lid lag
6. Palpate the neck
a. Stand behind and palpate bimanually
b. Describe size, shape, site, smoothness, symmetry, consistency,
fluctuance, tenderness, tethering. Thyroid specific – diffuse or
single. Smooth or multinodular. Could offer to transluminate
(cysts).
c. Palpate asking patient to stick tongue out and swallow water
d. Palpate for lymph nodes
e. Palpate for centrally located trachea
7. Percuss retrosternally for retrosternal goitre
8. Auscultate for thyroid bruit while patient holds their breath(very
suggestive of Grave’s)
9. Legs
a. Inspect for pretibial myxoedema
12. http://www.youtube.com/watch?v=krXoyP5j5lk - St. George’s thyroid exam
b. Ask patient to hold arms out like a chicken against resistance
and stand from sitting with their arms crossed– proximal
myopathy (hypothyroidism)
c. Test reflexes. Brisk = hyper, slow=hypo
10. Thank the patient, offer to help them get dressed
11. Wash hands