1. 1 | P a g e
Gatheredby: AbdulmalikAl-Ghamdi, NassirAl-Saeed, AbdulrahmanAbu-Khashba, ,SaudKhan
SalihAshgar, Mustafa Al-Zaytooni, RaghadShawoosh.
Writtenby:Hawra Al-Eirani _Special ThanksGoesto: KhalidAlShabrawy
Cardiology
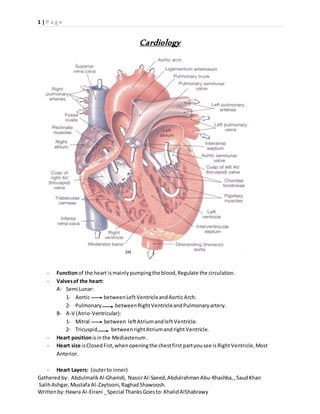
- Functionof the heart ismainlypumpingthe blood,Regulate the circulation.
- Valvesof the heart:
A- Semi Lunar:
1- Aortic betweenLeftVentricleandAorticArch.
2- Pulmonary betweenRightVentricleandPulmonaryartery.
B- A-V (Atrio-Ventricular):
1- Mitral between leftAtriumandleft Ventricle.
2- Tricuspid betweenrightAtriumandright Ventricle.
- Heart positionisinthe Mediastenum.
- Heart size isClosedFist,whenopeningthe chestfirst partyousee isRightVentricle,Most
Anterior.
- Heart Layers: (outerto inner)
2. 2 | P a g e
Gatheredby: AbdulmalikAl-Ghamdi, NassirAl-Saeed, AbdulrahmanAbu-Khashba, ,SaudKhan
SalihAshgar, Mustafa Al-Zaytooni, RaghadShawoosh.
Writtenby:Hawra Al-Eirani _Special ThanksGoesto: KhalidAlShabrawy
1- Pericardium.
2- Myocardium.
3- Endocardium.
- Collectionof Fluidinthe PericardiumcalledCardiacTemponae ( Doesn’tPumpWell).
- Circulationof the Blood:
Superior&InferiorVenaCava RightAtrium Right Ventricle Pulmonaryartery
Lung Pulmonaryvein Left Atrium Left Ventricle Aorta The Whole Body.
- Borders of the Heart:
1- Right Border:
a- Superior&InferiorVenaCava.
b- RightAtrium.
2- Left Border:
a- LeftAtrium& Ventricle.
b- PulmonaryArtery.
c- AorticArtery.
3- InferiorSurface:
a- RightVentricle.
b- Apex Left Ventricle.
- Blood Supplyto the heart isthe Coronary Arteries.
- AnyVeindrainsinthe RightAtrium.
- Bundle BranchBlock:meanssome of the Myocardiaumwill getthe Impulsesandthe restwill
not,still be relaxed.
- Controllingof BloodFlow: Valves:
1- During Systole:
a- A-V Closed.
b- Semi Lunar Opened.
2- During Diastole:
a- A-V Opened.
b- Semi Lunar Closed.
- Soundheardof the heartis Due to Closure of the Valves.
- S1 Sound[Closure of A-V] Systole Occurs S2 Sound[ Closure of Semi Lunar] Diastole Occurs
- All Myocardiumcellsworkasone cell Sensetium,incase of CardiacDamage,the damage
cell will release TroponinandMyocinintothe blood Knownas:Cardiac Markers.
3. 3 | P a g e
Gatheredby: AbdulmalikAl-Ghamdi, NassirAl-Saeed, AbdulrahmanAbu-Khashba, ,SaudKhan
SalihAshgar, Mustafa Al-Zaytooni, RaghadShawoosh.
Writtenby:Hawra Al-Eirani _Special ThanksGoesto: KhalidAlShabrawy
- ConductionSystem: [ SA AV Bundle Branch/ Purkinje fibers.]
- SA node isthe base makersendsimpulsestothe A-V,The A_V node waitsawhile before
sendingsothe Ventriclesrelax andgetfillewithbloodtocontract.Then,the A-V node sendsthe
ImpulsesThroughtthe Bundle Branchsthen,toPurkinje fibers.
- Cardiac Cycle :
- Stroke Volume = 70-80 ml ejectedwitheverybeat.
- Abnormal Sounds( MURMURS):
In Murmur:
a- Stenosis Soundheardwhenthe Valve isOPEN.
4. 4 | P a g e
Gatheredby: AbdulmalikAl-Ghamdi, NassirAl-Saeed, AbdulrahmanAbu-Khashba, ,SaudKhan
SalihAshgar, Mustafa Al-Zaytooni, RaghadShawoosh.
Writtenby:Hawra Al-Eirani _Special ThanksGoesto: KhalidAlShabrawy
b- Regarge Soundheardwhenthe Valve isCLOSED.
In A-VValves Diastole Open Stenosis.
Systole Closed Regergitation.
In Semi Lunar Valves Diastole Closed Regergitation.
Systole Open Stenosis
- ElectroCardioGram(ECG):
- Waves:
1- P Wave AtriumDepolarization(Anyproblemwithrightorleftatriumwill showin
thiswave inthe ECG).
2- QRS Complex Ventricle Depolarization,Atrium repolarization( The wave will show
the ImpulsesgoingthroughSeptal,Base,Apex of the heart.VentricularDepolarizationis
strongerthan Atrial Re-Polarization.
3- T Wave VentricularRe-Polarization.
- Segments:( Iso-ElectricLine)
1- ST Segment To IdentifyIschemia.
2- PR Segment For A-V Activity.
3- TP Segment For the Base Line.
- Interval: (Wave + Segment)
1- PR interval P wave + PR Segment.
2- QT interval QRS Complex +ST segment.
- In the ECG paper: 1 Big Square = 5 Small Square of 1 line.
Therefore,1Big Square = 0,2sec and 1 Small Square = 0,04sec.
- In 1 min 300 BigSquare.
- Heart Rate = 60-100 CountedfromR-Ronly1 Cycle (bigsquares).
- HR= 300/no. of squares.
- Rhythem betweenR-R( mustcompare between3-4cycles) (bigsquare)
5. 5 | P a g e
Gatheredby: AbdulmalikAl-Ghamdi, NassirAl-Saeed, AbdulrahmanAbu-Khashba, ,SaudKhan
SalihAshgar, Mustafa Al-Zaytooni, RaghadShawoosh.
Writtenby:Hawra Al-Eirani _Special ThanksGoesto: KhalidAlShabrawy
- Accessory Pathway Abnormalities:
1- P-R Interval: Normallytakes3-5Small Square.
- Can be short or prolong.
Short Abnormalities:
a- WolfParkinsonWhite Syndrome (WPW):
I. Short P-RSegment.
II. Slurring(Deltawave).
III. Wide QRS
b- Lown Ganong Levine Syndrome (LGL):A-V SendsImpulse Directly
I. Short P-Rsegment.
Prolong Abnormalities:(HeartBlock),[We lookbetweenR-R]
a- 1st
Degree DelayedConductionThoughthe A-V node (All arrive butdelayed)
Long PRsegment
6. 6 | P a g e
Gatheredby: AbdulmalikAl-Ghamdi, NassirAl-Saeed, AbdulrahmanAbu-Khashba, ,SaudKhan
SalihAshgar, Mustafa Al-Zaytooni, RaghadShawoosh.
Writtenby:Hawra Al-Eirani _Special ThanksGoesto: KhalidAlShabrawy
b- 2nd
Degree Half the impulse arrive andhalf dont
I. Wenckebach(Mobit1) Progressive (Hasspecificpatterns),getsworse
witheachcycle.
II. Mobit 2 2 cyclesare normal and1 abnormal (either2or 3 or 4).
c- 3rd
Degree (CompleteHeartBlock),norelationbetweenatriumandventricle.
VerylongPRsegment.
Alsoin3rd
degree,Insomecases,HeartDevlopan EctopicFoci.
Ectopic Foci: Ectopic foci are abnormal pacemaker sites within the heart
(outside of the SA node) that display automaticity, which can cause additional
beats (observed as premature beats) or take over the normal pacemaker
7. 7 | P a g e
Gatheredby: AbdulmalikAl-Ghamdi, NassirAl-Saeed, AbdulrahmanAbu-Khashba, ,SaudKhan
SalihAshgar, Mustafa Al-Zaytooni, RaghadShawoosh.
Writtenby:Hawra Al-Eirani _Special ThanksGoesto: KhalidAlShabrawy
activity of the SA node. These ectopic pacemakers can lead to
either tachycardia or bradycardia.
- Bundle Branch block: Anybundle branchblockresultin (Wide QRS).
1- QRS ComplexAbnormalities: relatedtothe ventricle,QRSisnormallynarrow.
a- Left VentricularHypertrophy:
We lookat V1 = DeepS wave
V6 = Tall R wave
8. 8 | P a g e
Gatheredby: AbdulmalikAl-Ghamdi, NassirAl-Saeed, AbdulrahmanAbu-Khashba, ,SaudKhan
SalihAshgar, Mustafa Al-Zaytooni, RaghadShawoosh.
Writtenby:Hawra Al-Eirani _Special ThanksGoesto: KhalidAlShabrawy
To say the patientishypertrophicV1+V6 = 35 andabove
( we count‘S’ bigSquares Longitudinally,and‘R’bigsquaresLongitudinally,each
multipliedin5thenaddedtogether)
b- Right VentricularHypertrophy: Tall R,we onlyneedtolookat V1 and V2.
- Lead Placement:
a. ChestLeads:
b. Limb lead + Bipolar Leads( bipolarisconnectionbetween2leads):
9. 9 | P a g e
Gatheredby: AbdulmalikAl-Ghamdi, NassirAl-Saeed, AbdulrahmanAbu-Khashba, ,SaudKhan
SalihAshgar, Mustafa Al-Zaytooni, RaghadShawoosh.
Writtenby:Hawra Al-Eirani _Special ThanksGoesto: KhalidAlShabrawy
- AxisDeviation (heartposition):we lookat Lead1 + AVF(foot) =we lookat QRS.
a. Left AxisDeviation:
b. Right Axis Deviation:
c. Odd AxisDeviation: Bothlead1 and leadAVFwill be pointingdownwards.
Lead 1 Lead aVF
Right Axis Deviation -ve (pointingdownward) +ve (pointingupwards)
Left AxisDeviation +ve (pointingupwards) -ve (pointingdownward)
Odd AxisDeviation -ve (pointingdownward) -ve (pointingdownward)
- Bundle Branch Block: we lookat V1,V6 lead.
a. Left Bundle Branch Block (LBBB):
10. 10 | P a g e
Gatheredby: AbdulmalikAl-Ghamdi, NassirAl-Saeed, AbdulrahmanAbu-Khashba, ,SaudKhan
SalihAshgar, Mustafa Al-Zaytooni, RaghadShawoosh.
Writtenby:Hawra Al-Eirani _Special ThanksGoesto: KhalidAlShabrawy
V1 noR QS pattern.
V6 Tall,Wide R lookslike M.
b. Right Bundle Branch Block:
V1 M Shape R’ Wide.
V6 W shape S Wide.
- Heart Sound:
a. First Sound (S1) Mitral and Tricuspidclosure In isovolumetricSystole.
b. SecondSound (S2) Aorticand Pulmonaryclosure In Diastole.
c. Third and fourth Sound (S3, S4) Pathological
I. Third Sound (S3): Rapidventricularfilling,presentinheartfailure.
11. 11 | P a g e
Gatheredby: AbdulmalikAl-Ghamdi, NassirAl-Saeed, AbdulrahmanAbu-Khashba, ,SaudKhan
SalihAshgar, Mustafa Al-Zaytooni, RaghadShawoosh.
Writtenby:Hawra Al-Eirani _Special ThanksGoesto: KhalidAlShabrawy
II. Fourth Sound (S4): Late diastole,associatedwithAtriumHypertrophy
Contraction.
d. OpeningSnap Mitral StenosisinDiastole.
e. Pericardial Knock TB in PeriCardiuminDiastole.
f. SystolicEjection Click AorticstenosisinSystole.
g. Mid Systolicclick Mitral vavle prolapse inSystole.
h. MetalicClick Prostheticvalve closure.
i. Splitand Fixed Atriumseptal defect.
- All Addedsoundsare heardinDiastole.
- Arrhythmia : Disterbance of heartbeatinconductionorimpulse orboth.
- Anyarrhythmiawe should:
1. Regularity.
2. QRS.
3. Rate.
- TachyCardia > 100
a. Regular:
I. Narrow QRS:
Supra-Ventricular: Originof conduction
i. SA node P wave.
ii. Atrium Ectobic Foci P-Wave Morphology.
iii. A-VNode if mainconductionisfromA-V NoP Wave.
iv. Atrium Flatter HR=300 Saw toothappearance.
Treatment: HemodynamicStability(BP):
If stable Base maker+ Medication.
If not stable Shock treatment.
II. Wide QRS:
i. SA node Normal Pwave.
ii. A-Vnode Bundle BranchBlock andEctobic Foci.
iii. Atrium Flatter Bundle BranchBlockand Ectobic Foci.
b. Irregular:
I. Aterial Fibrilation=600
II. VentricularFibrilation= 600
III. Treatment: Cardioversion:
If stable Medications.
If not stable Shock.
- In Tachycardia massage to the carotid bodywill stimulate VagusNervecausingBradycardia.
- All Arrhythmiawe use Synchronized ShockTreatment( ShockAfterQRScomplex) exceptVentricular
Treatmentnoneed,CausednoQRS complex inVF.
- Bradycardia:
12. 12 | P a g e
Gatheredby: AbdulmalikAl-Ghamdi, NassirAl-Saeed, AbdulrahmanAbu-Khashba, ,SaudKhan
SalihAshgar, Mustafa Al-Zaytooni, RaghadShawoosh.
Writtenby:Hawra Al-Eirani _Special ThanksGoesto: KhalidAlShabrawy
a. Regular:
I. QRS Narrow:
i. SA node P Wave Present.
ii. A-V node Mobit2
iii. IdioVentrecular Ectobic Foci in ventricle 3rd
degree.
II. QRS Wide:Bundle BranchBlockor EctobicFoci.
b. Irregular:
I. AF
II. AV
III. Treatment: Medication.
- Approach to Cardiac Patient:
- Symptoms of Heart Disease:
1. Chestpain
2. Dyspnea
3. Palpitation
4. Syncope
5. Fatigue
6. Peripheral Oedema
- Central Chest Pain: Painof AnginaPectorisandMyocardial Infarction Due to myocardial
Hypoxia.
a. Angina Retro-sternal heavyorgrippingsensation,withradiationtoleftorneck.
ProvokedbyExertion,easedbyrestof niterates.
b. Acute Coronary Syndrome SimilartoAnginapainbutat rest.
c. Aortic Dissection Severe tearingchestpain,radiatingtothe back.
d. Pericarditispain sharp central chestpain,worse whenmovingorrespirating.
Relievedbysittingforward.
e. Da Costa’s Syndrome Sharp, stabbing,leftsub-mammarypain.
Associatedwithanexity.
- Dyspnea: causedbyLeft ventricularfailure,due toOedemaof pulmonaryinterstitiumandalvioli.
a. Orthopnea Breathlessnessonlaying flat.
b. Parpxysmal nocturnal dyspnea Patientwakesfromsleepfightingforbreath.
c. Cheyne-stokesrespiration Hyperventilation+alternatingepisodesof apnea
Heart failure.
d. Central sleepapnea syndrome (CSAS) hypopneaandapneatogethercalled
“Periodicbreathing”.
- Syncope:lossof consciousness, due toinadequate cerebral bloodflow.
a. Vascular:
13. 13 | P a g e
Gatheredby: AbdulmalikAl-Ghamdi, NassirAl-Saeed, AbdulrahmanAbu-Khashba, ,SaudKhan
SalihAshgar, Mustafa Al-Zaytooni, RaghadShawoosh.
Writtenby:Hawra Al-Eirani _Special ThanksGoesto: KhalidAlShabrawy
I. Vasovagal attack simple Faint(mostCommon).
II. Postural (Orthostatic) hypotension drop of systolicpressure within2
hoursof eating.
III. Micturitionsyncope lossof consciousnesswhile passingurine.
IV. Carotidsinussyncope whenthere isexaggeratedvagal response to
carotidsinusstimulation,aggravatedbywearingtightcollarorlooking
upwardsor turningthe head.
b. Obstructive:due to restrictionof bloodflow fromthe heartto the restof the
circulation,orbetweenthe heartchampers.
c. Arrhythmias: stokes-adamattacks suddenlossof consciousness,unrelatedto
posture,pulse usuallyslow orabsent.
- Fatigue:inadequate systemicperfusion of heartfailure,due topoorsleepordirectside effectof
medication: a. beta-blocker. b. electrolyticimbalance.
- Periphral Oedema: heartfailure resultinsaltandwaterretention,whichleadtodependentpitting
Oedema.
- Palpitation:increase awarenessof normal heartbeator sensationof slow,rapidorirregularheart
rhythms:
a. Pre-mature beats: pause followedbyforcefulbeat.
b. Paroxysmal tachycardias: Suddenracingheartbeats.
c. Brady Cardias: slow,regular,heavyorforceful beats.
![2 | P a g e
Gatheredby: AbdulmalikAl-Ghamdi, NassirAl-Saeed, AbdulrahmanAbu-Khashba, ,SaudKhan
SalihAshgar, Mustafa Al-Zaytooni, RaghadShawoosh.
Writtenby:Hawra Al-Eirani _Special ThanksGoesto: KhalidAlShabrawy
1- Pericardium.
2- Myocardium.
3- Endocardium.
- Collectionof Fluidinthe PericardiumcalledCardiacTemponae ( Doesn’tPumpWell).
- Circulationof the Blood:
Superior&InferiorVenaCava RightAtrium Right Ventricle Pulmonaryartery
Lung Pulmonaryvein Left Atrium Left Ventricle Aorta The Whole Body.
- Borders of the Heart:
1- Right Border:
a- Superior&InferiorVenaCava.
b- RightAtrium.
2- Left Border:
a- LeftAtrium& Ventricle.
b- PulmonaryArtery.
c- AorticArtery.
3- InferiorSurface:
a- RightVentricle.
b- Apex Left Ventricle.
- Blood Supplyto the heart isthe Coronary Arteries.
- AnyVeindrainsinthe RightAtrium.
- Bundle BranchBlock:meanssome of the Myocardiaumwill getthe Impulsesandthe restwill
not,still be relaxed.
- Controllingof BloodFlow: Valves:
1- During Systole:
a- A-V Closed.
b- Semi Lunar Opened.
2- During Diastole:
a- A-V Opened.
b- Semi Lunar Closed.
- Soundheardof the heartis Due to Closure of the Valves.
- S1 Sound[Closure of A-V] Systole Occurs S2 Sound[ Closure of Semi Lunar] Diastole Occurs
- All Myocardiumcellsworkasone cell Sensetium,incase of CardiacDamage,the damage
cell will release TroponinandMyocinintothe blood Knownas:Cardiac Markers.](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)