2. Acute infection of the soft tissues of the orbit behind
the orbital septum
May/may not progress to a subperiosteal/orbital
abscess
3. Etiology
Modes of infection
Exogenous infection
Result from penetrating injury
Extension of infection from
neighbouring structures
Paranasal sinuses, teeth,
face, lids, intracranial cavity,
intraorbital structures
Endogenous infection
Rarely develop as metastatic
infection from breast
abscess,etc.
Causative organisms
Streptococcus pneumoniae
Staphylococcus aureus
Streptococcus pyogenes
Haemophilus influenzae
4. Pathology
Similar to suppurative inflammations of the body in
general except:
• d/t absence of lymphatics in the orbit
Infection establishes early
• Infections spreads as thrombophebitis from surrounding
structures
Rapid spread with extensive necrosis
• As orbital infection is ass. With raised intraorbital pressure
d/t tight compartment
Damage produced is rapid and extensive
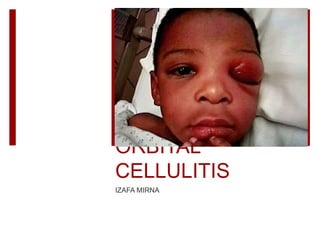
5. CLINICAL FEATURES
Symptoms
Swelling and severe pain (increased by movements of
eyeball/pressure)
Ass. General symptoms- fever, nausea, vomiting &
prostrations
Visual loss &/ diplopia in moderate to advanced disease
6. Signs
Swelling of lids (woody hardness
& redness)
Chemosis of conjunctiva (protrude
& become desiccated/necrotic)
Axial proptosis
Restriction of ocular movements
(mild-severe)
RAPD –complications in the form
of optic neuropathy/CRAO
Fundus examination –congestion
of retinal veins,
papillitis/papilloedema)
7. COMPLICATIONS
Ocular complications
* Exposure keratopathy
* Optic neuritis
* CRAO
Orbital complications
* Subperiosteal abscess
* Orbital abscess
Temporal/parotid abscess
*d/t spread of infection
around the orbit
Intracranial complications
* Carvenous sinus
thrombosis
* Meningitis
* Brain abscess
General
septicemia/pyaemia
8. • Collection of purulent material between the
orbit bony wall & periosteum
• Suspected when associated with eccenteric
proptosis
• Confirm by CT scan
Subperiosteal
abscess
• Collection of pus within orbital tissue
• Suspected by signs of severe proptosis,
marked chemosis, complete
ophthalmoplegia & pus point below
conjunctiva
• Confirm by CT scan
Orbital
abscess
9. INVESTIGATIONS
Bacterial cultures
From nasal and conjunctival swabs and blood samples
Complete haemogram
May reveal leukocytosis
X-ray PNS
Identify associated sinusitis
Orbital ultrasonography
Detect intraorbital abscess
CT scan & MRI
Differentiating preseptal & postseptal cellulitis
Detect subperiosteal abscess
Orbital abscess
Intracranial extension
Deciding when & where to drain orbital abscess
10. TREATMENT
Orbital cellulitis is an emergency!
Hospitalised the patient for aggressive management
1. Intensive antibiotic therapy
• Staph infections: high doses of
penicillinase-resistant
antibiotics+ampicillin
• Alternative: cefotaxime,
ciprofloxacin, vancomycin
• H. influenzae : chloramphenicol /
clavulanic acid
• Anaerobes : oral metronidazole
500mg every 8 hours
2. Analgesic & anti-inflammatory
drugs
• control pain and fever
3. Topical antibiotic eye ointment
• QID, for corneal exposure and
chemosis (severe proptosis)
4. Start nasal decongestant drops
5. Revaluation
• 2-3 times/day
• to monitor the response and modify
the Rx accordingly
11. Surgical intervention
Indications:
Unresponsiveness to antibiotics
Decrease vision
Presence of an orbital/subperiosteal abscess
Immediate canthotomy / cantholysis
If the orbit is tight, presence of optic neuropathy, IOP severely
elevated.
Free incision into the abscess
When presence under skin or conjunctiva.
Drainage of pus
For subperiosteal abscess : 2-3 cm curved incision in upper medial
aspect.
Drain both orbit and infected paranasal sinuses.