2. Contents
• Introduction
• Development of cementum
• Molecular factors affecting cementogenesis
• Physical properties
• Chemical composition
• Histology of cementum
• Classification
• Cemento-dentinal junction
• Cemento-enamel junction
3. Contents
• Functions
• Cementum resorption and repair
• Effects of ageing on cementum
• Cementum in oral environment
• Role of cementum in periodontal disease
• Changes in cementum
• Developmental anomalies
• Conclusion
• References
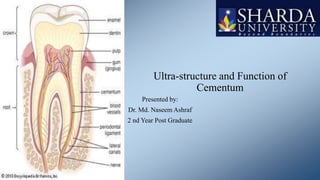
4. Introduction
• Definition: calcified avascular mesenchymal tissue that forms the outer covering of the anatomic
roots
• Extent: begins at cervical portion of the tooth at the cemento-enamel junction up to the apical
foramen
• First demonstrated microscopically in 1835 by Franke and Rashkow (two pupils of purkinje)
• Anatomically – part of tooth
• Functionally- part of periodontium
5. Development of Cementum
Initiation
HERS- Corono-apical
extension of IEE and
OEE induces
secretion of enamel
proteins
Facing
ectomesenchymal
cells of dental papilla
differentiate into the
odontoblast
HERS becomes
interupted and
ectomesenchymal
cells of inner portion
of dental follicle
comes in contact with
the pre-dentin
Odontoblasts starts
forming pre-dentin
Em cells of follicle
receive signal from
dentin and
surrounding HERS
cells & differentiate
into cementoblasts
6.
7.
8. Physical Characteristics
• Hardness: less than dentin
• Colour: Light yellow with dull surface and lighter than dentin
• Thickness: Variable, thinnest at CEJ and thickest at at apex. Apical foramen is surrounded by
cementum
• Its permeable, (as age progresses permeability of cementum diminishes)
9. Chemical characteristics
• On dry weight basis, cementum of fully formed teeth contains:
• Inorganic substances- 45-50%
• Organic substances and water- 50-55%
10. Inorganic Portion
• Hydroxyapatite- calciumand Phosphate
• Trace elements like
- Copper
- Flourine
- Iron
- Lead
- Potassium
- Silica
• Cementum has highest fluorine content among mineralized tissues
11. Organic portion
• Collagen: Type I predominant (90%), others include type III (5%), V, XII, XIV
• Matrix proteins
• Proteoglycans
• Osteonectin
• Osteopontin
• Osteocalcin
• Fibronectin
• Bone sialoprotein
12. Organic portion
• Protein extracts of mature cementum
• Promotes cell attachment and migration
• Stimulates protein synthesis for gingival fibroblasts and PDL cells
• Bone sialoprotein & osteopontin
• Differentiation of progenitor cells to cementoblasts
13. Histology of cementum
• Histology section of cementum shows:
• A) Cells, fibers, ground substance
• B) Cemento-enamel junction
• C) Cemento-dentinal junction
14. Histology of Cementum
• Cells of cementum
• The cells associated with cementum are:
• Cementoblast
• Cementocytes
• Cementoclasts
15. Histology of cementum
• CEMENTOBLASTS
• Numerous mitochondria
• Well defined golgi apparatus
• Large number of granular endoplasmic reticulum
• Synthesise collagen and protein polysaccharide, which make up the organic matrix of cementum
• After some cementum is laid down, its mineralisation begins
• The cells are found lining the root
16. Histology of Cementum
• CEMENTOCYTES
• Spider shaped cells, characteristic feature of cellular cementum
• During the formation of cellular cementum, cemetoblasts
become entrapped within their own matrix due to rapid
deposition and are called cementocytes
• Similar to osteocytes, they lie in spaces called as lacunae
• Haphazardly arranged and widely dispersed
• In deeper layers of cementum, cementocytes shows definite
signs of degeneration such as cytoplasmic clumping, empty
lacunae, vesiculation
17. Histology of cementum
• CEMENTOCLASTS
• Found in howship’s lacunae
• Unilocular/multilocular cells
• Function: resorption of cementocytes
• Major role: resorption and repair
18. Histology of cementum
• INCREMENTAL LINES OF CEMENTUM
• Refered to as incremental lines of salter
• Represent rhythmic periodic deposition of cementum
• Appears as dark lines running parallel to root surface
• Seen in both cellular and acellular cementum but more prominent in acellular cementum
• Best seen in decalcified sections under light microscope
• Highly mineralized areas with less collagen and more ground substance
20. Types of cementum
• By location:
• 1) Radicular cementum
• 2) Coronal cementum
• By cellularity:
• 1) Cellular cementum
• 2) Acellular cementum
• By the presence of collagen fibrils in the matrix:
• 1) Fibrillar cementum
• 2) Afibrillar cementum
• A/c to development
• Primary (prefunctional )
• Secondary (functional)
21. Types of Cementum
• By the origin of matrix fibers:
• 1) Extrinsic fibers
• 2) Intrinsic fibers
• 3) Mixed fibers
22. Types of Cementum
• ACELLULAR CEMENTUM
• First to be formed
• Covers cervical 3rd or half of the root
• Does not contain cells
• Formed before tooth reaches occlusal plane
• Thickness 30-230 μm
• Composed mostly of sharpey’s fibers
• Contains intrinsic calcified collagen fibrils
25. Types of Cementum
• CELLULAR CEMENTUM
• Secondary formed cementum
• Contains cementocytes
• Formed after tooth reaches the occlusal plane
• Less calcified than acellular cementum
• Thicker than acellular cementum
• Sharpey’s fibers occupies a smaller portion
28. Based on nature and origin of organic matrix
• 2 sources of collagen
extrinsic intrinsic
Extrinsic fibers-known as sharpey’s fibers-embedded portion of Principle fibers of PDL
Formed by fibroblast
Intrinsic fibers- belong to cementum
Formed by cementoblast
Cementoblast also forms non-collagenous proteins like glycoproteins, proteoglycans etc
30. Acellular Afibrillar Cementum
• Contains neither cells nor intrinsic or extrinsic fibers
• Product of cementoblast , found at coronal cementum
• Thickness 1-1.5 micrometer
• Lacks collagen and hence plays no role in attachment
• Deposited on enamel and dentine in close proximity to CEJ
31. Acellular Extrinsic Fiber Cementum
• Composed of densely packed bundles of sharpey’s fibers & lacks cells
• Product of fibroblast and cementoblast
• Found in cervical third of root-may extend apically
• Thickness between 30-230 micrometer
• Only type of cementum seen in single rooted teeth
• Cementoid is not found
• Main function is anchorage- specially in single rooted teeth
32. Cellular Mixed Stratified Cementum
• Composed of extrinsic and intrinsic fibers and cells
• Co-product of fibroblast and cementoblast
• Appears in apical third of roots, apices and in furcation areas
• Thickness 100-1000 micrometers
• Intrinsic fibers are uniformly mineralised but the extrinsic fibers are variably mineralised with
some central unmineralised zones
33. Cellular Intrinsic Fiber Cementum
• Contains cells and intrinsic fibers
• Formed by cementoblast and fills resorption lacunae
• Majority of fibers are organised parallel to the root surface
• Cells have phenotype of bone forming cells
• Very minor role in attachment
• Corresponds to cellular cementum and is seen in middle to apical third and inter-radicular
cementum
34. Intermediate cementum
• Ill defined cementum near CEJ of certain teeth
• Contains cellular remnants of Hertwig's epithelial root sheath
• Embedded in calcified ground substance
• Thickness is 10 micrometers
35. Cemento-Dentinal Junction
• Interface between cementum and dentine
• In deciduous teeth- scalloped
• In permanent teeth- smooth
• Areas of dentine adjacent to CDJ appears granular in ground section due to colaescing and looping
of terminal portion of dentinal tubules and is called TOMES GRANULAR LAYER
• During RCT obturating material must end near CDJ
• No increase or decrease in width with age(2-3 micrometer)
38. Cemento-enamel Junction
• Functions:
• Provide medium for attachment to collagen fibers of the PDL
• Cementum is harder than alveolar bone and is avascular and doesn’t show resorption under
masticatory or orthodontic forces
• Thus during orthodontic forces tooth integrity is maintained and alveolar bone being elastic in
nature changes its shape, fulfilling orthodontic requirement
• Functions as covering for root surface
• Cementum has the property of continuous deposition thus it repairs
damage such as fracture or root resorption
• Cementum can aid in maintaining the teeth in functional occlusion
if deposited in apical aspect in patients with chronic bruxism- passive eruption
39. Cementum Resorption and Repair
• Permanent teeth doesn’t undergo the process of physiologic resorption as does the counterpart
• However the cementum of erupted as well as unerupted teeth is subject to resorptive changes
that may be of microscopic proportion or sufficiently extensive to present a radiographically
detectable alteration in the root contour
• Local conditions
• 1) Trauma from ocllusion
• 2) Orthodontic movement
• 3) Cysts and Tumours
• 4) Pressure from malaligned erupted teeth
• 5) Peri-apical disease and Periodontal disease
Systemic Conditions
1) Paget’s disease
2) Hypothyroidism
3) Heridity fibrous osteodystrophy
4) Calcium deficiency
40. Cementum Resorption and Repair
• Cementum resorption appear microscopically as bay like concavities in the
root surface
• Multi-nucleated giant cells and large mononuclear macrophages are
generally found adjacent to cementum undergoing active resorption
• Several sites of resorption coalesce to form a larger area of destruction
• Resorptive process may extend into underlying dentin and even into pulp,
but its usually painless
• Cementum resorption is not necessarily continuous and may alternate with
periods of repair and deposition of new cementum
• The newly formed cementum is demarcated from the root by a deep
stained irregular line, termed as reversal line, which delineates the border
of the previous resorption
41. Cementum Resorption and Repair
• Repair of cementum is a process to heal the damage caused by resorption or cemental fracture
• Cementum repair requires the presence of viable connective tissue
• If epithelium proliferates in the area of resorption then repair will not take place
• Repair can occur in both vital and non-vital teeth
• Repair can be
Anatomical Functional
42. Cementum Resorption and Repair
• Anatomic Repair: The root outline is re-established as it was before
cemental resorption. It generally occurs when the degree of destruction is low
• Cementum resorption is repaired by cellular and acellular cementum
• Functional Repair: in cases of large cemental resorption or destruction,
repair doesn’t re-establish the same contour as before
• To maintain the width of PDL, the adjacent alveolar bone grows and takes the
shape of defect, this is done to improve the function of tooth, hence called
functional repair
43.
44. Effect of Ageing on Cementum
• With ageing the surface of cementum becomes more
irregular. This is caused by calcification of some fiber
bundles where they were attached to cementum
• Cemental width may increase with increasing age (5-10
times)
• Increase in width is greater apically and lingually
• In ageing, a continuous increase of cementum in the apical
zone may result in obstruction of apical foramen
45. Exposure of Cementum to oral environment
• Cementum becomes exposed to oral cavity in cases of gingival
recession and a consequence of loss of attachment in pocket
formation
• Cementum is sufficiently permeable to be penetrated by micro-
organisms, organic and inorganic substances in such cases
• Bacterial invasion of the cementum occurs commonly in periodontal
disease
• Caries of cementum can also develop
46. Role of Cementum in Periodontal disease
The surface on
which plaque and
calculus attach.
Role of therapy is
to remove these
accretions as a part
of treatment plan
It forms the inner
wall of
periodontal
pocket
This tissue is static
as compared to
other dynamic
tissues in the
surrounding, so
any change will
have long term
effects
Its intimately
involved in all
phases of
Periodontal
disease processes,
so it must be
returned to a
healthy state
DCNA Vol.24 Issue 4 (1980)- Joseph J. Aleo
47. Changes in Cementum Associated with
Periodontal Disease
• Structural Changes
• Partial demineralization
• Repreciation of dissolved minerals
• Decrease or loss of cross banding of collagen
• Sub-surface condensation of organic material of exogenous origin
• Chemical Changes
• Increase in calcium and phosphate levels
• Increase in fluoride content
• Decrease in sodium levels
48. Changes in Cementum Associated with Periodontal Disease
• Cytotoxic changes
• Effects on cell proliferation
• Hatfield and Bomhammers- inhibitory substance penetrates the exposed cementum that
prevents growth of epithelial cells in tissue cultures
• Presence of endotoxins - limits fibroblast proliferation – detrimental to the arrest of disease
• Cementum bound endotoxins – 50 times more toxic
• Destructive physical changes – cavitation, partial demineralisation
• Effect on cell attachment
• Cultured human gingival fibroblasts do not attach to diseased tooth (Aleo etal 1975)
49. Changes in Cementum Associated with Periodontal Disease
• Inhibitory principle of matrix- Morris (1975)
• Disease inhibited development of implanted marrow whereas demineralised healthy tooth did not
• Demineralised diseased roots showed more inhibition-toxins must have seeped into root matrix
during pocket formation and demineralization removed the toxin allowing development of marrow
• According to inhibitory principle of matrix-phenol extraction usually required to remove toxins
from bacterial cell wall is not necessary to make diseased cementum receptive cell attachment
50. Changes in Cementum Associated with Periodontal Disease
• In early and moderate periodontitis- acellular cementum is affected (coronal half of the root)
• Damage extends to cellular cementum in most advanced periodontal conditions and furcally
positioned lesions
• These surfaces are almost always covered by cellular cementum during successful regeneration,
whether this is adequate is unclear (McNeil and Sommerman-1999)
51. Role of Cementum Molecules in Periodontal
Regeneration
• Growth factors and adhesion molecules present in cementum are also active towards cells of
gingiva, PDL and alveolar bone (Narayanan and Bartold-1996; Bartold etal-2000)
• Its possible that these growth factors present have the potential to participate in the regeneration of
these tissues
• But its not significant as growth factors remain bound within cementum matrix
• Even if inflammatory component releases them, their relative concentrations are likely to be less
than those available from blood and inflammatory cells
• Therefore contributions of cementum molecules towards regeneration of other periodontal tissues
are likely to remain marginal
52. Chemical Modifications of Cementum
• Addition of zinc to cultures relieved endotoxin induced depression of cellular proliferation
• Chelation of zinc enhanced cellular toxicity of endotoxin-Aleo
• Studies analyzing effect of zinc on cellular attachment are still underway
• Register & Burddick- tested effects of partial demineralization by acid on attachment (Dog models)
• Results-production of cementum pins- reattachment with cementogenesis- repair of chronic
interproximal defects- complete alveolar bone repair over labial defects by 1 year
55. Developmental Anomalies of Cementum
• Enamel Projections
• If amelogenesis does not stop before the start of root
formation, enamel may continue to form over portions
normally covered by cementum
• Enamel Pearls
• This consist of globules of enamel on root surface in
cervical regeneration (act as plaque retentive areas)
56. Developmental Anomalies of Cementum
• Hypercementosis
• Refers to prominent thickening of cementum
• It may be localised to one tooth or may involve the entire
dentition (Paget’s disease)
• Occurs as generalised thickening of the cementum, with nodular
enlargement of cementum in apical third of root
• Etiology of Hypercementosis
• Spike-like type of hypercementosis: results from excessive
forces from orthodontic appliances or occlusal forces
• Generalised type-occurs in teeth without antagonist
57. Developmental Anomalies of Cementum
• Cementoblastoma
• Only neoplasm of cementum
• Cementum like tissue is deposited around the roots of teeth as
irregular or rounded mass
• Age less than 25
• Involves commonly- mandibular molars and pre-molars
• Tooth usually as vital pulp
• Attached to roots and causes its resorption, involves pulp
canal and also causes slow expansion of cortical plate
• Enlargement produced is usually asymptomatic
58. Developmental Anomalies of Cementum
• Cementicles
• Are small, globular masses of cementum found in approx
35% of human roots.
• May not be always attached to the cementum surface but
may be located free in Pdl.
• These may result from microtrauma, when extra stress on
sharpey’s fibers causes a tear in the cementum.
• Are more commonly found in apical & middle third of root
and in root furcation areas
• May develop from calcified epithelial rests; around small
spicules of cementum or alveolar bone traumatically
displaced into the periodontal ligament;
• from calcified Sharpey's fibers; and from calcified,
thrombosed vessels within the periodontal ligament
59. Developmental Anomalies of Cementum
• Cementoma
• Benign cementoblastoma/cemental dysplasia
• Represents an unusual reaction of bone
• Caused due to occlusal trauma
• Present usually at apex of mandibular incisor
• Almost exclusiely found in black persons
• Age-20 to 40 years
• Causes expansion of jaw
60. Developmental Anomalies of Cementum
• Concrescence
• Form of fusion which occurs root formation has been
completed
• Thought to arise as a result of crowding or traumatic injury
of the teeth with resorption of interdental bone so that the
two roots are in approximate contact and fused by deposition
of cementum between them
• May occur before or after tooth has erupted
61. Developmental Anomalies of Cementum
• Cementopathia
• In 1923, Gottlieb reported a fatal case of influenza and
he attributed it as atrophy of bone
• Characterised by loss of collagen in PDL and their
replacement by loose connective tissues and bone
resorption resulting in widened PDL space
• Gottlieb attributed this condition to inhibition of
continuous cementum formation which he considered
essential for cementum formation
• He then termed the disease as cementopathia
62. Developmental Anomalies of Cementum
• Hypophosphatasia
• This is a hereditary disease characterised by total absence
of cementum
• It results in early loss of teeth
• It occurs due to deficiency of enzyme alkaline phosphatase
(ALP )in serum and tissues
63. Developmental Anomalies of Cementum
• Ankylosis
• Fusion of alveolar bone and cementum with obliteration of
PDL space is termed as ankylosis
• Occurs in cases of cemental resorption, may represent a
form of abnormal repair
• May develop after chronic apical inflammation, tooth re-
plantation and occlusal trauma
• Results in resorption of root and gradual replacement with
bone tissue
64. • Cemental tears
• The detachment of a fragment of cementum is
described as a cemental tear. Cemental tears
have been reported in the periodontal literature
associated with localized, rapid periodontal
breakdown.
65. Conclusion
• Cementum is an important tissue of the periodontium, attachment apparatus of the
tooth and helps in tooth movements
• Cementum deposition is continuous process but this tissue is rather static as
compared to the surrounding dynamic tissue therefore it hast be taken into account
while performing various dental procedures
• Although the morphogenesis and the established structure of the various cementum
varieties have been described by many researchers, knowledge of cementum
physiology still lags behind what is known about the other dental and periodontal
tissues. The interest in cementum, however, has never been given up by researchers,
and the ultimate goal of true periodontal regeneration after treatment for
periodontitis has revived vigorously the interest in this unique mineralized tissue
66. References
• Carranza’s clinical periodontology (10th & 11th edition)
• Orban’s –Text Book Of Oral Histology And Embryology 11th edition
• Mallar KB, Girish HC, Murgod S, Yathindra Kumar BN. Age estimation using annulations in
root cementum of human teeth: A comparison between longitudinal and cross sections. J
Oral Maxillofac Pathol 2015;19:396-404
• Alistair D King, Tamer Turk, Canan Colak, Selma Elekdag-Turk, Allan S. Jones, Peter Petocz
Ali M. Physical properties of root cementum: Part 21.Extent of root resorption after the
application of 2.5 degrees and 15 degrees tips for 4 weeks: A microcomputed tomography
study. Am J Orthod Dentofacial Orthop 2011;140:e299-e305
• Higgins D, Kaidonis J, Townsend G, Hughes T, Austin J. Targeted sampling of cementum for
recovery of nuclear DNA from human teeth and the impact of common decontamination
measures. Investigative Genetics 2013, 4:18
• Boscchardt D, Selvig K. Dental Cementum: The dynamic tissue covering the root surface.
Periodontology 2000. Vol. 13, 1997, 41-75